Text A Acute Appendicitis
Incidence and Epidemiology
With more than250,000appendectomies performed annually,appendicitis is the most common abdominal surgical emergency in the United States.The peak incidence of acute appendicitis is in the second and third decades of life;it is relatively rare at the extremes of age.However,perforation is more common in infancy and in the elderly,during which periods mortality rates are highest.Males and females are equally affected,except between puberty and age 25,when males predominate in a 3∶2 ratio.The incidence of appendicitis has remained stable in the United States over the last 30 years,while the incidence of appendicitis is much lower in underdeveloped countries,especially parts of Africa,and in lower socioeconomic groups.The mortality rate in the United States decreased eightfold between 1941 and 1970 but has remained at<1 per 100,000since then.
Pathogenesis
Appendicitis(Fig.11-1,11-2)is believed to occur as a result of appendiceal luminal obstruction.Obstruction is most commonly caused by a fecalith,which results from accumulation and inspissation of fecal matter around vegetable fibers.Enlarged lymphoid follicles associated with viral infections(e.g. measles),inspissated barium,worms(e.g.pinworms,Ascaris and Taenia),and tumors(e.g.carcinoid or carcinoma)may also obstruct the lumen.Other common pathological findings include appendiceal ulceration.The cause of the ulceration is unknown,although a viral etiology has been postulated.Infection with Yersinia organisms may cause the disease,since high complement fixation antibody titers have been found in up to 30%of cases of proven appendicitis. Luminal bacteria multiply and invade the appendiceal wall as venous engorgement and subsequent arterial compromise result from the high intraluminal pressures. Finally,gangrene and perforation occur.If the process evolves slowly, adjacent organs such as the terminal ileum,cecum,and omentum may wall off the appendiceal area so that a localized abscess will develop,whereas rapid progression of vascular impairment may cause perforation with free access to the peritoneal cavity.Subsequent rupture of primary appendiceal abscesses may produce fistulas between the appendix and bladder,small intestine,sigmoid,or cecum. Occasionally,acute appendicitis may be the first manifestation of Crohn disease.
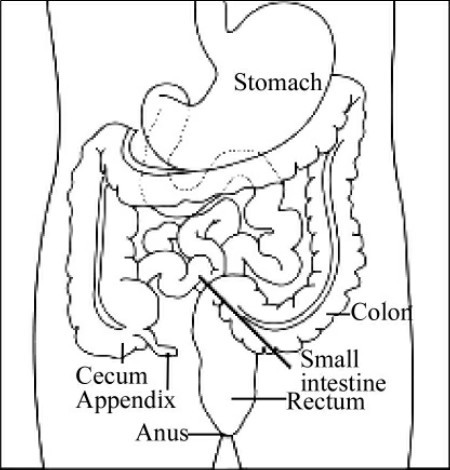
Fig.11-1 Diagram of the appendix
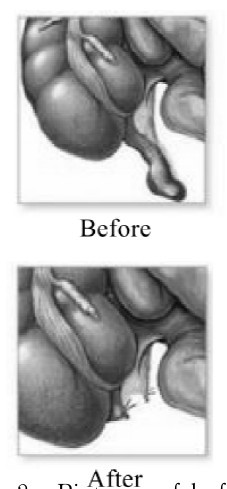
Fig.11-2 Pictures of before and after operation on the inflamed appendix
While chronic infection of the appendix with tuberculosis,amebiasis,and actinomycosis may occur,a useful clinical aphorism states that chronic appendiceal inflammation is not usually the cause of prolonged abdominal pain of weeks'or months'duration.
Clinical Manifestation
The sequence of abdominal discomfort and anorexia associated with acute appendicitis is pathognomonic.The pain is described as being located in the periumbilical region initially and then migrating to the right lower quadrant. This classic sequence of symptoms occurs in only 66%of patients.However,in a male patient these symptoms are sufficient to advise surgical exploration.The periumbilical abdominal pain is of the visceral type,resulting from distention of the appendiceal lumen.In general,this visceral pain is mild,often cramping and usually lasting 4—6 h.
As inflammation spreads to the parietal peritoneal surfaces,the pain becomes somatic,steady,and more severe and aggravated by motion or cough. Parietal afferent nerves are A delta fibers,which are fast-conducting and unilateral.These fibers localize the pain to the right lower quadrant.Anorexia is very common;a hungry patient does not have acute appendicitis.Nausea and vomiting occur in 50%—60%of cases,but vomiting is usually self-limited.
Change in bowel habit is of little diagnostic value,since any or no alteration may be observed,although the presence of diarrhea caused by an inflamed appendix in juxtaposition to the sigmoid may cause diagnostic difficulties.Urinary frequency and dysuria occur if the appendix lies adjacent to the bladder.Physical findings vary with time after onset of the illness and according to the location of the appendix,which may be situated deep in the pelvic cul-de-sac;in the right lower quadrant in any relation to the peritoneum, cecum,and small intestine;in the right upper quadrant(especially during pregnancy);or even in the left lower quadrant.
The diagnosis cannot be established unless tenderness can be elicited.While tenderness is sometimes absent in the early visceral stage of the disease,it ultimately always develops and is found in any location corresponding to the position of the appendix.Typically,tenderness to palpation will often occur at Mc Burney's point,anatomically located on a line one-third of the way between the anterior iliac spine and the umbilicus.Abdominal tenderness may be completely absent if a retrocecal or pelvic appendix is present,in which case the sole physical finding may be tenderness in the flank or on rectal or pelvic examination.Referred rebound tenderness is often present and is most likely to be absent early in the illness.Flexion of the right hip and guarded movement by the patient are due to parietal peritoneal involvement.Hyperesthesia of the skin of the right lower quadrant and positive psoas or obturator sign are often late findings and are rarely of diagnostic value.
The temperature is usually normal or slightly elevated,but a temperature>38.3℃should suggest perforation.Tachycardia is commensurate with the elevation of the temperature.Rigidity and tenderness become more marked as the disease progresses to perforation and localized or diffuse peritonitis.
Distention is rare unless severe diffuse peritonitis has developed.A mass may develop if localized perforation has occurred but will not usually be detectable before 3 days after onset.Earlier presence of a mass suggests carcinoma of the cecum or Crohn disease.Perforation is rare before 24 h after onset of symptoms,but the rate may be as high as 80%after 48 h.
Leukocytosis of>20×109cells/L suggests probable perforation.Anemia and blood in the stool suggest a primary diagnosis of carcinoma of the cecum, especially in elderly individuals.The urine may contain a few white or red blood cells without bacteria if the appendix lies close to the right ureter or bladder.Urinalysis is most useful in excluding genitourinary conditions that may mimic acute appendicitis.
Infants under 2 years of age have a 70%—80%incidence of perforation and generalized peritonitis.This is thought to be the result of a delay in diagnosis.Any infant or child with diarrhea,vomiting,and abdominal pain is highly suspect.Fever is much more common in this age group,and abdominal distention is often the only physical finding.In the elderly,pain and tenderness are often blunted,and thus the diagnosis is also frequently delayed and leads to a30%incidence of perforation in patients over 70 years.Elderly patients often present initially with a slightly painful mass or with adhesive intestinal obstruction5 or 6 days after a previously undetected perforated appendix.
Appendicitis occurs about once in every 500—2,000pregnancies and is the most common extrauterine condition requiring abdominal operation.The diagnosis may be missed or delayed because of the frequent occurrence of mild abdominal discomfort and nausea and vomiting during pregnancy and because of the gradual shift of the appendix from the right lower quadrant to the right upper quadrant during the second and third trimester of pregnancy.Appendicitis tends to be most common during the second trimester.The diagnosis is best made with ultrasound,which has an 80%accuracy;however,if perforation has already occurred,the accuracy of ultrasound decreases to 30%.Early intervention is warranted because the incidence of fetal loss with a normal appendix is 1.5%.With perforation,the incidence of fetal loss is 20%—35%.
Differential Diagnosis
Acute appendicitis has been labeled masquerader,and the diagnosis is more difficult to make in the young females.Obtaining agood history,including sexual activity and the presence of a vaginal discharge,will help differentiate acute appendicitis from pelvic inflammatory disease(PID).The presence of a malodorous vaginal discharge and gram-negative intracellular diplococci are pathognomonic for PID.Pain on movement of the cervix is also more specific for PID but may occur in appendicitis if perforation has occurred or if the appendix lies adjacent to the uterus or adnexa.Rupture of a graafian follicle occurs at midcycle and will produce pain and tenderness more diffuse and usually of a less severe degree than in appendicitis.Rupture of a corpus luteum cyst is identical clinically to rupture of a graafian follicle but develops about the time of menstruation.The presence of an adnexal mass,evidence of blood loss, and a positive pregnancy test help differentiate ruptured tubal pregnancy. Twisted ovarian cyst and endometriosis are occasionally difficult to distinguish from appendicitis.In all these female conditions,ultrasonography and laparoscopy may be of great value.
Acute mesenteric lymphadenitis and acute gastroenteritis are the diagnosis usually given when enlarged,slightly reddened lymph nodes at the root of the mesentery and a normal appendix are encountered at operation in a patient who usually has right lower quadrant tenderness.Retrospectively,these patients may have had a higher temperature,diarrhea,more diffuse pain and abdominal tenderness,and a lymphocytosis.Between cramps,the abdomen is completely relaxed.Children seem to be affected more frequently than adults.Some of these patients have infection with Y.pseudotuberculosis or Y.enterocolitis,in which case the diagnosis can be established by culture of the mesenteric nodes or by serologic titers.In Salmonella gastroenteritis,the abdominal findings are similar,although the pain may be more severe and more localized,and fever and chills are common.Regional enteritis is usually associated with a more prolonged history,often with previous exacerbations regarded as episodes of gastroenteritis unless diagnosis has been established previously.Often an inflammatory mass is palpable.In addition,acute cholecystitis,perforated ulcer,acute pancreatitis,acute diverticulitis,strangulating intestinal obstruction, ureteral calculus,and pyelonephritis may present diagnostic difficulties.
Treatment
If the diagnosis is in question,4—6 h of observation with serial abdominal exams is always more beneficial than harmful.Antibiotics should not be administered when the diagnosis is in question,since they will only mask the perforation.The treatment of presumed acute appendicitis is early operation and appendectomy as soon as the patient can be prepared.Appendectomy is frequently accomplished laparoscopically and is associated with less postoperative narcotic use and earlier discharge.It is acceptable to have a 15%—20%incidence of a normal appendix at the time of appendectomy to avoid perforation.The use of early laparoscopy instead of close clinical observation has not shown a clinical benefit in the management of patients with nonspecific abdominal pain.
A different approach is indicated if a palpable mass is found 3—5 days after the onset of symptoms.This finding usually represents the presence of a phlegmon or abscess,and complications from attempted surgical excision are frequent.Such patients treated with broad-spectrum antibiotics,drainage of abscesses>3 cm,parenteral fluids,and bowel rest usually show resolution of symptoms within1 week.Interval appendectomy can be performed safely 6—12 weeks later.A randomized clinical trial has demonstrated that antibiotics alone can effectively treat acute,nonperforated appendicitis in86%of male patients.However,antibiotics alone were associated with a higher recurrence rate than surgical intervention.If the mass enlarges or the patient becomes more toxic, the abscess should be drained.Perforation is associated with generalized peritonitis and its complications,including subphrenic,pelvic,or other abscesses,and can be avoided by early diagnosis.The mortality rate for nonperforated appendicitis is 0. 1%,little more than the risk of general anesthesia;for perforated appendicitis,mortality is 3%(and can reach 15%in the elderly).
(1,874 words)
New Words and Phrases
appendicitis[ə,pendɪ'saɪtɪs]n. 阑尾炎
epidemiology['epɪ,diːmɪ'ɒlədʒɪ]n. 流行病学
appendectomy[,æpen'dektəmɪ]n. 阑尾切除术
appendiceal[æpen'dɪsɪəl]a. 阑尾的
inspissation[,ɪnspɪ'seɪʃən]n. 蒸浓法;浓缩法
fecal['fiːkəl]a. 粪便的
fecalith['fiːkəlɪθ]n. 粪石
lymphoid['lɪmfɒɪd]a. 淋巴的,淋巴样的
viral['vaɪrəl]a. 病毒的
postulate['pɒstjʊleɪt]n. 假定v. 假定;要求
Yersinia[jзː'sɪnɪə]n. 耶尔森鼠疫杆菌
titer['taɪtə,'tiː-]n. 滴度,效价
engorgement[ɪn'ɡɔːdʒmənt]n. 充血;肿胀
terminal ileum 末端回肠;回肠末端
cecum['siːkəm]n. (同于caecum)盲肠
omentum[əʊ'mentəm]n. 网膜
wall off 堵塞壁缝
peritoneal[,perɪtəʊ'niːəl]a. 腹膜的
fistula['fɪstjʊlə]n. 瘘管
bladder['blædə]n. 膀胱;囊状物
sigmoid['sɪɡmɒɪd]n. 乙状结肠a. 乙状结肠的
Crohn disease 克罗恩病,节段性回肠炎
amebiasis[,æmɪ'baɪəsɪs]n. 阿米巴病
actinomycosis[,æktɪnəʊmaɪ'kəʊsɪs]n. 放射菌病
aphorism['æfərɪzəm]n. 格言,警句
periumbilical[,perɪəm'bɪlɪkəl]a. 脐周的
quadrant['kwɒdrənt]n. 象限,四分体,扇形体
visceral['vɪsərəl]a. 内脏的
somatic[səʊ'mætɪk]a. 躯体的
afferent['æfərənt]a. 传入的,输入的
delta['deltə]n. 三角形区,丁种
unilateral[,juːnɪ'lætərəl]a. 单侧的;一侧的
juxtaposition[,dʒʌkstəpə'zɪʃən]n. 并置,并列
cul-de-sac['kʌldə'sæk]n. (法)盲管,陷凹
elicit[ɪ'lɪsɪt]v. 引出;引起
palpation[pæl'peɪʃən]n. 触诊;扪诊
Mc Burney's point 麦氏点
anatomically[,ænə'tɒmɪkəlɪ]ad. 解剖学上
iliac['ɪlɪæk]a. 髂的;髂骨的
umbilicus[ʌm'bɪlɪkəs]n. 脐
retrocecal[,retrəʊ'siːkəl]a. 盲肠后的
flank[flæŋk]n. 侧面;肋腹v. 位于……的侧面
rectal['rektəl]a. 直肠的
flexion['flekʃən]n. 屈曲;屈
hyperesthesia[,haɪpəriːs'θiːzɪə]n. 感觉过敏
psoas['psəʊəs]n. 腰(大)肌
obturator['ɒbtjʊəreɪtə]n. 充填器;闭孔肌
commensurate[kə'menʃərət]a. 相称的,同量的
peritonitis[,perɪtə'naɪtɪs]n. 腹膜炎
genitourinary[,dʒenɪtəʊ'jʊərɪnərɪ]a. 泌尿生殖器的
extrauterine[,ekstrə'juːtəraɪn]a. (位于或发生在)子宫外的
warrant['wɒrənt,'wɔː-]n. 根据;证明
malodorous[mæl'əʊdərəs]a. 有恶臭的
Gram-negative['ɡræm'neɡətɪv]a. 革兰阴性的
intracellular[,ɪntrə'seljʊlə]a. 细胞内的
diplococci[,dɪpləʊ'kɒksaɪ]([复]diplococcus)n. 双球菌
adnexa[æd'neksə]n. 附件
Graafian follicle 格拉夫卵泡,囊状卵泡
corpus['kɔːpəs]n. 体
cyst[sɪst]n. 囊肿;(包)囊
corpus luteum cyst 黄体囊肿
adnexal[æd'neksəl]a. 附件的
lymphadenitis[lɪm,fædɪ'naɪtɪs]n. 淋巴结炎
mesentery['mesəntərɪ,mez-]n. 肠系膜
lymphocytosis[,lɪmfəʊsaɪ'təʊsɪs]n. 淋巴细胞增多(症)
pseudotuberculosis['psjuːdəʊtjʊ,bзːkjʊ'ləʊsɪs]n. 假结核病
enterocolitis[,entərəʊkə'laɪtɪs]n. 小肠结肠炎
Y.enterocolitis 小肠结肠炎耶尔森菌
serologic[,sɪərə'lɒdʒɪk]a. 血清学的
Salmonella[,sælmə'nelə]n. 沙门菌属
gastroenteritis[,ɡæstrəʊ,entə'raɪtɪs]n. 肠胃炎
enteritis[,entə'raɪtɪs]n. 肠炎
palpable['pælpəbl]a. 明显的;可感知的
cholecystitis[,kɒlɪsɪs'taɪtɪs]n. 胆囊炎
ulcer['ʌlsə]n. 溃疡;腐烂物
pancreatitis['pænkrɪə'taɪtɪs]n. 胰腺炎
diverticulitis[daɪvə,tɪkjʊ'laɪtɪs]n. 憩室炎
ureteral[jʊ'riːtərəl]a. 输尿管的
pyelonephritis[,paɪələʊnɪ'fraɪtɪs,-ne-]n. 肾盂肾炎
laparoscopy[,læpə'rɒskəpɪ]n. 腹腔镜检查
calculus['kælkjʊləs]n. 结石
narcotic[nɑː'kɒtɪk]n. 麻醉药,镇静剂a. 麻醉的
phlegmon['fleɡmɒn]n. 蜂窝织炎
subphrenic[sʌb'frenɪk]a. 膈下的
anesthesia[ænɪs'θiːzɪə]n. 麻醉;麻木
 Exercises
Exercises
Ⅰ.Reading Comprehension
A.Answer the following questions.
1.What is it believed that causes appendicitis?
2.Why is change in bowel habit of little diagnostic value?
3.What is the temperature when perforation is suggested?
4.What will help differentiate acute appendicitis from pelvic inflammatory disease in young females?
5.Why should antibiotics not be administered when diagnosis of appendicitis is in question?
B.Choose the right answer to each question.
1.Where does the pain of appendicitis migrate to when it is initially located in the peri-umbilical region?
A.The pain is located in the periumbilical region initially and then migrates to the right upper quadrant.
B.The pain is located in the periumbilical region initially and then migrates to the left upper quadrant.
C.The pain is located in the periumbilical region initially and then migrates to the right lower quadrant.
D.The pain is located in the periumbilical region initially and then migrates to the left upper quadrant.
2.Where is Mc Burney's point,when tenderness to palpation often occurs?
A.Mc Burney's point is anatomically located on a line a half of the way between the anterior iliac spine and umbilicus.
B.Mc Burney's point is anatomically located on a line one-third of the way between the anterior iliac spine and umbilicus.
C.Mc Burney's point is anatomically located on a line two-thirds of the way between the anterior iliac spine and umbilicus.
D.Mc Burney's point is anatomically located on a line one-fifth of the way between the anterior iliac spine and umbilicus.
3.How many cells of Leukocytosis suggest probable perforation?
A.Leukocytosis of over 20×109cells/L suggests probable perforation.
B.Leukocytosis of over 30×109cells/L suggests probable perforation.
C.Leukocytosis of over 40×109cells/L suggests probable perforation.
D.Leukocytosis of over 50×109cells/L suggests probable perforation.
4.What is most useful in excluding genitourinary conditions that mimic acute appendicitis?
A.Physical examination is most useful.
B.Blood test is most useful.
C.Stool test is most useful.
D.Urinalysis is most useful.
5.How many weeks later can interval appendectomy be performed safely?
A.6—12 weeks later. B.A month later.
C.3 weeks later. D.10 days later.
Ⅱ.Words and Expressions
A.Fill in the blanks with the words or expressions given below,and change the form where necessary.
tenderness appendectomy colon antibody pelvic
appendix inflammation cecum nausea abscess
urinalysis antibiotics bacteria laparoscopy peritonitis
1.The appendix is a small,worm-like appendage attached to the__________ .
2.Appendicitis occurs when bacteria invade and infect the wall of the__________ .
3.The most common complications of appendicitis are abscess and__________ .
4.The most common symptoms of appendicitis are abdominal pain,loss of appetite,nausea and vomiting,fever,and abdominal__________ .
5.Due to the varying size and location of the appendix and the proximity of other organs to the appendix,it may be difficult to differentiate appendicitis from other abdominal and__________ diseases.
6.The treatment for appendicitis usually is antibiotics and__________ .
7.Complications of appendectomy include wound infection and__________ .
8.It is thought that appendicitis begins when the opening from the appendix into the__________ becomes blocked.
9.An alternative theory for the cause of appendicitis is an initial rupture of the appendix followed by spread of__________ outside of the appendix.
10.The inflammation,pain and symptoms may disappear.This is particularly true in elderly patients and when__________ are used.
B.Fill in the blanks with the suitable words or expressions from each group.
On the basis of experimental evidence,acute appendicitis seems to be the end result of a primary 1 of the appendix lumen.Once this obstruction occurs,the appendix subsequently becomes filled with 2 and swells, increasing pressures within the lumen and the walls of the appendix,resulting in 3 and occlusion of the small vessels,and stasis of 4 flow.Rarely, spontaneous recovery can occur at this point.As the former progresses,the appendix becomes 5 and then necrotic.As bacteria begin to leak out through the dying walls, 6 forms within and around the appendix.The end result of this cascade is 7 rupture causing 8 ,which may lead to septicemia(败血症)and eventually death.
The causative agents include foreign bodies,trauma, 9 worms,lymphadenitis, and,most commonly, 10 fecal deposits known as appendicoliths or fecaliths.The occurrence of obstructing fecaliths has attracted attention since their presence in patients with appendicitis is significantly higher in developed than in developing countries,and an appendiceal 11 is commonly associated with complicated appendicitis.Also,fecal 12 and arrest may play a role,as demonstrated by a significantly lower number of 13 movements per week in patients with acute appendicitis compared with healthy controls.The occurrence of a fecalith in the 14 seems to be attributed to a right-sided fecal retention reservoir in the 15 and a prolonged transit time. From 16 data,it has been stated that diverticular(憩息的)disease and adenomatous polyps(腺瘤性息肉)were unknown and colon cancer exceedingly rare in communities exempt for 17 .Also,acute appendicitis has been shown to occur antecedent to cancer in the colon and 18 .Several studies offer evidence that a low fiber intake is involved in the 19 of appendicitis This is in accordance with the occurrence of a right-sided 20 reservoir and the fact that dietary fiber reduces transit time.
1.A.damage B.wound C.obstruction D.pressure
2.A.node B.strand C.cramp D.mucus
3.A.thrombosis B.follicle C.fecal D.rupture
4.A.rectal B.sigmoid C.lymphatic D.appendiceal
5.A.luminal B.peritoneal C.ischemic D.visceral
6.A.pus B.blood C.tear D.dirty
7.A.lymphoid B.appendiceal C.viral D.genitourinary
8.A.peritonitis B.cholecystitis C.lymphadenitis D.pancreatitis
9.A.umbilical B.intestinal C.ovarian D.adnexal
10.A.palpable B.toxic C.ectopic D.calcified
11.A.follicle B.cecum C.fecalith D.bladder
12.A.stasis B.abscess C.inflammation D.stump
13.A.bowel B.viral C.recurrent D.ureteral
14.A.calculus B.psoas C.bladder D.appendix
15.A.fistula B.colon C.cervix D.mesentery
16.A.chemical B.epidemiological C.physical D.biological
17.A.appendicitis B.pancreatitis C.gastritis D.enteritis
18.A.abdomen B.gastrin C.rectum D.uterus
19.A.etiology B.puberty C.pathogenesis D.calculus
20.A.epigastric B.serologic C.lymphoid D.fecal
Ⅲ.Translation
A.Translate the following sentences into Chinese.
1.Appendicitis is believed to occur as a result of appendiceal luminal obstruction.Obstruction is most commonly caused by a fecalith,which results from accumulation and inspissation of fecal matter around vegetable fibers.
2.Physical findings vary with time after onset of the illness and according to the location of appendix,which may be situated deep in the pelvic cul-de-sac;in the right lower quadrant in any relation to the peritoneum,cecum, and small intestine;in the right upper quadrant(especially during pregnancy);or even in the left lower quadrant.
3.In addition,acute cholecystitis,perforated ulcer,acute pancreatitis,acute diverticulitis,strangulating intestinal obstruction,ureteral calculus,and pyelonephritis may present diagnostic difficulties.
B.Translate the following sentences into English.
1.急性阑尾炎的典型症状首先是疼痛,随后呕吐,最后发烧。由于阑尾神经分布延伸至第10节胸椎脊髓,与脐部位置相平行,所以疼痛始于腹中部。之后,随着阑尾炎症状加重并刺激邻近腹腔壁,数小时后疼痛往往会集中于右下腹。
2.根据实验结果,阑尾管腔原发性梗阻似乎最终都会诱发急性阑尾炎。一旦阑尾管腔发生阻塞,阑尾内就会充满黏液并肿胀,使腔内和管壁压力上升,导致小血管形成血栓,发生阻塞并使淋巴流动停滞。
Ⅳ.Writing
A.Write an abstract of Text A.
B.Write a topic-related and literature-based report on Appendicitis.