Text A Bronchiectasis
Bronchiectasis is an abnormal and permanent dilatation of bronchi.It may be either focal,involving airways supplying a limited region of pulmonary parenchyma,or diffuse,involving airways in a more widespread distribution.It is a disorder that typically affects older individuals,approximately two-thirds of patients are women.
Pathology
The bronchial dilatation of bronchiectasis is associated with destructive and inflammatory changes in the walls of airways,often at the level of segmental or subsegmental bronchi.The normal structural components of the wall,including cartilage,muscle,and elastic tissue,are destroyed and may be replaced by fibrous tissue.The dilated airways frequently contain pools of thick,purulent material,while more peripheral airways are often occluded by secretions or obliterated and replaced by fibrous tissue.Additional microscopic features include bronchial and peribronchial inflammation and fibrosis, ulceration of the bronchial wall,squamous metaplasia,and mucous gland hyperplasia.The parenchyma normally supplied by the affected airways is abnormal, containing varying combinations of fibrosis,emphysema,bronchopneumonia, and atelectasis.As a result of the inflammation,vascularity of the bronchial wall increases,with associated enlargement of the bronchial arteries and anastomoses between the bronchial and pulmonary arterial circulations.
Etiology and Pathogenesis
Bronchiectasis is a consequence of inflammation and destruction of the structural components of the bronchial wall.Infection is the usual cause of the inflammation; microorganisms such as Pseudomonas aeruginosa and Haemophilus influenzae produce pigments,proteases,and other toxins that injure the respiratory epithelium and impair mucociliary clearance.The host inflammatory response induces epithelial injury,largely as a result of mediators released from neutrophils.As protection against infection is compromised,the dilated airways become more susceptible to colonization and growth of bacteria. Thus,a reinforcing cycle can result,with inflammation producing airway damage,impaired clearance of microorganisms,and further infection,which then completes the cycle by inciting more inflammation.
Infectious Causes
Adenovirus and influenza virus are the main viruses that cause bronchiectasis in association with lower respiratory tract involvement.Virulent bacterial infections, especially with potentially necrotizing organisms such as Staphylococcus aureus,Klebsiella,and anaerobes,remain important causes of bronchiectasis when antibiotic treatment of a pneumonia is not given or is significantly delayed.Infection with Bordetella pertussis,particularly in childhood,has also been associated with chronic suppurative airways disease.Tuberculosis,a major cause of bronchiectasis worldwide,can produce airway dilatation by a necrotizing effect on pulmonary parenchyma and airways and indirectly as a consequence of airway obstruction from bronchostenosis or extrinsic compression by lymph nodes.Nontuberculous mycobacteria are frequently cultured from patients with bronchiectasis,often as secondary infections or colonizing organisms.
Impaired host defense mechanisms are often involved in the predisposition to recurrent infections.The major cause of localized impairment of host defenses is endobronchial obstruction.Bacteria and secretions cannot be cleared adequately from the obstructed airway,which develops recurrent or chronic infection. Slowly growing endobronchial neoplasms such as carcinoid tumors may be associated with bronchiectasis.Foreign-body aspiration is another important cause of endobronchial obstruction,particularly in children.Airway obstruction can also result from bronchostenosis,from impacted secretions,or from extrinsic compression by enlarged lymph nodes.
Generalized impairment of pulmonary defense mechanisms occurs with immunoglobulin deficiency,primary ciliary disorders,or cystic fibrosis. Infections and bronchiectasis are therefore often more diffuse.
Noninfectious Causes
Some cases of bronchiectasis are associated with exposure to a toxic substance that incites a severe inflammatory response.Examples include inhalation of a toxic gas such as ammonia or aspiration of acidic gastric contents,though the latter problem is often also complicated by aspiration of bacteria.An immune response in the airway may also trigger inflammation, destructive changes,and bronchial dilatation.This mechanism is presumably important for bronchiectasis with allergic bronchopulmonary aspergillosis (ABPA),which is due at least in part to an immune response to Aspergillus organisms that have colonized the airway.Inα1-antitrypsin deficiency,the usual respiratory complication is the early development of panacinar emphysema,but affected individuals may occasionally have bronchiectasis.
Clinical Manifestations
Patients typically present with persistent or recurrent cough and purulent sputum production.Repeated,purulent respiratory tract infections should raise clinical suspicion for bronchiectasis.Hemoptysis occurs in 50%—70%of cases and can be due to bleeding from inflamed airway mucosa.More significant, even massive bleeding is often a consequence of bleeding from hypertrophied bronchial arteries.Systemic symptoms such as fatigue,weight loss,and myalgias can also occur.
When a specific infectious episode initiates bronchiectasis,patients may describe a severe pneumonia followed by chronic cough and sputum production. In some cases,patients are either asymptomatic or have a nonproductive cough,often associated with“dry”bronchiectasis in an upper lobe.Dyspnea or wheezing generally reflects either widespread bronchiectasis or underlying chronic obstructive pulmonary disease.With exacerbations of infection,the amount of sputum increases,and it becomes more purulent and often more bloody;systemic symptoms,including fever,may also be prominent.
Physical examination of the chest overlying an area of bronchiectasis is quite variable.Any combination of crackles,rhonchi,and wheezes may be heard,all of which reflect the damaged airways containing significant secretions.With other types of chronic intrathoracic infection,clubbing may be present.Patients with severe diffuse disease,particularly those with chronic hypoxemia,may have associated cor pulmonale and right ventricular failure.
Radiographic and Laboratory Findings
Though the chest radiograph is important in the evaluation of suspected bronchiectasis,the findings are often nonspecific.At one extreme,the radiograph may be normal with mild disease.Alternatively,patients with saccular bronchiectasis may have prominent cystic spaces,either with or without air-liquid levels,corresponding to the dilated airways.These may be difficult to distinguish from enlarged airspaces due to bullous emphysema or from regions of honeycombing in patients with severe interstitial lung disease. Other findings are due to dilated airways with thickened walls,which result from peribronchial inflammation.These dilated airways are often crowded together in parallel.When seen longitudinally,the airways appear as“tram tracks”;when seen in cross-section,they produce“ring shadows”.Because the dilated airways may be filled with secretions,the lumen may appear dense, producing an opaque tubular or branched tubular structure(Fig.7-1).
CT,especially with high-resolution images 1.0—1.5 mm thick,provides an excellent view of dilated airways(Fig.7-2).Consequently,it is now the standard technique for detecting or confirming the diagnosis of bronchiectasis.

Fig.7-1 X-ray image showing bronchiectasis
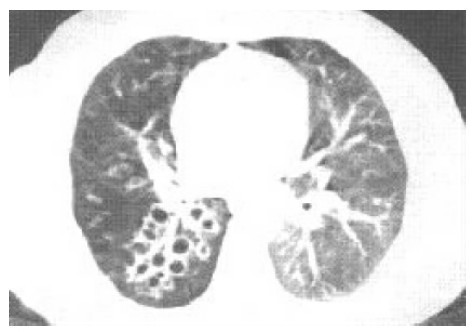
Fig.7-2 CT image showing bronchiectasis
Treatment
For patients with infrequent exacerbations characterized by an increase in quantity and purulence of the sputum,antibiotics are used only during acute episodes.Although choice of an antibiotic should be guided by Gram's stain and culture of sputum,empiric coverage(e.g.with amoxicillin,trimethoprim-sulfamethoxazole,or levofloxacin)is often given initially.
A variety of mechanical methods and devices accompanied by appropriate positioning can facilitate drainage in patients with copious secretions. Aerosolized recombinant DNase decreases viscosity of sputum by breaking down DNA released from neutrophils.Bronchodilators to improve obstruction and aid clearance of secretions are particularly useful in patients with airway hyperreactivity and reversible airflow obstruction.
When bronchiectasis is localized and the morbidity is substantial despite adequate medical therapy,surgical resection of the involved region of lung should be considered.
(1,160 words)
New Words and Phrases
bronchiectasis[,brɒŋkɪ'ektəsɪs]n. (细)支气管扩张(症)
dilatation[,daɪlə'teɪʃən]n. 扩张,扩张术
bronchus['brɒŋkəs]([复]bronchi)n. 支气管;小支气管
diffuse[dɪ'fjuːz]a. 弥漫的
bronchial['brɒŋkɪəl]a. 支气管的;细支气管的
inflammatory[ɪn'flæmətərɪ]a. 发炎的,炎性的
segmental[seɡ'mentəl]a. 段的
subsegmental[,sʌbseɡ'mentəl]a. 亚段的
purulent['pjʊrələnt]a. 脓的,化脓的
peribronchial[perɪ'brɒŋkɪəl]a. 支气管周的
fibrosis[faɪ'brəʊsɪs]n. 纤维化
ulceration[,ʌlsə'reɪʃən]n. 溃疡
squamous['skweɪməs]a. 鳞状的
metaplasia[,metə'pleɪzjə]n. 化生
hyperplasia[,haɪpə'pleɪzjə]n. 增殖,增生
emphysema[,emfɪ'siːmə]n. 肺气肿
bronchopneumonia[,brɒŋkəʊnjuː'məʊnjə]n. 支气管肺炎
atelectasis[,ætə'lektəsɪs]n. 肺不张,肺膨胀不全
vascularity[,væskjʊ'lærɪtɪ]n. 多血管(状态),血管分布
Pseudomonas[,psjuːdəʊ'məʊnəs]n. 假单胞菌属
aeruginosa[ɪəruː'dʒɪnəsə]n. 铜绿菌素
Pseudomonas aeruginosa 铜绿假单胞菌
Haemophilus[hiː'mɔːfɪləs]n. 嗜血杆菌属
influenza[ɪnflʊ'enzə]([复]influenzae)n. 流行性感冒(流感)
Haemophilus influenza 流感嗜血杆菌
pigment['pɪɡmənt]n. 色素
protease['prəʊtɪeɪz]n. 蛋白酶
toxin['tɒksɪn]n. 毒素
epithelium[,epɪ'θiːlɪəm]n. 上皮
mucociliary[,mjuːkəʊ'sɪlɪərɪ]a. 黏膜纤毛的
epithelial[,epɪ'θiːlɪəl]a. 上皮的
neutrophil['njuːtrəfɪl]n. 中性粒细胞
susceptible[sə'septəbl]a. 易感的,易受影响的
adenovirus['ædənəʊ,vaɪrəs]n. 腺病毒
virulent['vɪrjʊlənt]a. 致命的;(微生物)有毒力的
necrotize['nekrətaɪz]v. (使)坏死
Staphylococcus aureus[,stæfɪləʊ'kɒkəs'ɔːrɪəs] 金黄色葡萄球菌
Klebsiella[,klebzɪ'elə]n. 克雷白杆菌属
anaerobe[æ'neərəʊb]n. 厌氧菌
Bordetella[,bɔːdeɪ'telə]n. 包特杆菌属
pertussis[pзː'tʌsɪs]n. 百日咳
Bordetella pertussis 百日咳杆菌
suppurative['sʌpjəreɪtɪv]a. 化脓的
tuberculosis[tjuː,bзːkjʊ'ləʊsɪs]n. 结核病
bronchostenosis['brɔːŋkəʊstə'nəʊsɪs]n. 支气管狭窄
lymph[lɪmf]n. 淋巴
nontuberculous[,nɒntjuː'bзːkjʊləs]a. 无结节的;无结核的
mycobacteria[,maɪkəʊbæk'tɪərɪə]n. 分枝杆菌
endobronchial[,endəʊ'brɒŋkɪəl]a. 支气管内的
carcinoid['kɑːsɪnɒɪd]a. 良性肿瘤的n. 良性肿瘤
tumor['tjuːmə]n. 肿瘤
immunoglobulin[,ɪmjuːnəʊ'ɡlɒbjʊlɪn]n. 免疫球蛋白
cystic['sɪstɪk]a. 囊的;囊性的
ammonia[ə'məʊnjə]n. 氨,氨水
antitrypsin[,æntɪ'trɪpsɪn]n. 抗胰蛋白酶
panacinar[pæn'æsɪnə]a. 全叶性的
sputum['spjuːtəm]n. 痰;唾液
hemoptysis[hɪ'mɒptɪsɪs]n. 咯血
mucosa[mjuː'kəʊsə]n. 黏膜
myalgia[maɪ'ældʒɪə]n. 肌痛
lobe[ləʊb]n. (肺的)叶
dyspnea['dɪspnɪə]n. 呼吸困难
wheeze[hwiːz]v. 气喘n. 喘鸣,哮鸣音
exacerbation[ek,sæsə'beɪʃən]n. 恶化;加剧
rhonchus['rɔŋkəs]([复]rhonchi)n. 干啰音
intrathoracic[,ɪntrəθə'ræsɪk]a. 胸内的
clubbing['klʌbɪŋ]n. 杵状指
cor pulmonale['kɔː,pʊmə'nælɪ] 肺源性心脏病(肺心病)
saccular['sækjʊlə]a. 囊的
bullous['bʊləs]a. 大疱的,大泡的
opaque[əʊ'peɪk]a. 不透明的
empiric[em'pɪrɪk]a. 凭经验的
amoxicillin[ə,mɒksə'sɪlɪn]n. 阿莫西林
trimethoprim-sulfamethoxazole 复方磺胺甲 唑
唑
[traɪ'meθəʊprɪm,sʌlfəmeθ'ɒksəzəʊl]
levofloxacin[liːvəʊ'flɔːksəsɪn]n. 左氧氟沙星
DNase[,diːen'eɪz](deoxyribonuclease)n. 脱氧核糖核酸酶
 Exercises
Exercises
Ⅰ.Reading Comprehension
A.Answer the following questions.
1.What are the pathological characteristics of bronchiectasis?
2.As infection is the usual cause of the inflammation,what is the infection of bronchiectasis manifested?
3.Among the essential causes of bronchiectasis,what are the typical viruses and bacteria?
4.Can any symptom of hemoptysis,cough or purulent sputum production be used as the evidence in the evaluation of bronchiectasis and a severe pneumonia?Why?
5.Which treatment is considered effective in different cases of bronchiectasis?
B.Choose the right answer to each question.
1.Which of the following is NOT a correct statement about bronchiectasis?
A.Bronchiectasis may be either focal or diffuse.
B.Bordetella pertussis,as a main cause of bronchiectasis,often affects old people and women.
C.Bronchiectasis is caused by inflammation and destruction of the structural components of the bronchial wall.
D.Bronchiectasis is associated with immunoglobulin deficiency,primary ciliary disorders,or cystic fibrosis.
2.Bronchial fibrosis is caused by__________ .
A.the normal structural components of the wall,including cartilage, muscle,and elastic tissue
B.the abnormal parenchyma containing varying combinations of fibrosis
C.destructive and inflammatory changes in the walls of airways
D.the purulent material and the increase of vascularity of the bronchial wall
3.Which can be excluded from the main infectious causes of bronchiectasis?
A.Pseudomonas aeruginosa,Haemophilus influenzae and neutrophils.
B.Adenovirus,influenza virus and anaerobes.
C.Staphylococcus aureus,Klebsiella and anaerobes.
D.Bordetella pertussis,tuberculosis and Nontuberculous mycobacteria.
4.The following symptoms concerning bronchiectasis are all true EXCEPT that__________ .
A.patients often present with repeated,purulent respiratory hemoptysis
B.fatigue,weight loss,and myalgias can also occur
C.patients may be either asymptomatic or have a nonproductive cough
D.any combination of rhonchi and wheezes may be heard and dyspnea or wheezing possibly appears
5.Based on the information about radiographic and laboratory findings,we can infer that__________ .
A.all patients with bronchiectasis may have prominent cystic spaces
B.saccular bronchiectasis results from enlarged airspaces due to bullous emphysema
C.an opaque tubular or branched tubular structure produces dilated airways with thickened walls
D.the chest radiograph is often not specific in the evaluation of suspected bronchiectasis
Ⅱ.Words and Expressions
A.Fill in the blanks with the words or expressions given below,and change the form where necessary.
dilatation epithelium neutrophil respiratory bronchitis
pulmonary purulent inhalation wheeze hemoptysis
diffuse sputum secretion emphysema cystic
1.Bronchiectasis is characterized by permanent__________ of bronchi and bronchioles(细支气管).
2.__________ ,which refers to coughing up blood or blood-stained mucus usually,indicates a severe infection of the bronchi or lungs.
3.A flu infection thins the lining of the__________ tract,making the lungs more vulnerable to bacteria that can cause pneumonia.
4.The damaged airways make a lot more mucus than normal which forms__________ (phlegm).
5.The respiratory__________ ,the lining of the airway,serves as a leak-proof barrier that transports,filters and conditions the air we breathe.
6.During__________ ,the diaphragm becomes taut and pulls downward while the muscles between the ribs contract and pull upward.
7.The enterovirus in throat__________ and saliva of the patient may be transmitted to others via breathing droplets.
8.Bronchiectasis most commonly presents as a focal process involving a lobe, segment,or subsegment of the lung.Far less commonly,it may be a__________ process involving both lungs.
9.The bronchi supply air and__________ arteries supply blood to the lungs. Together they take in air from the atmosphere,oxygenate the blood,and excrete the carbon dioxide back out of the body.
10.The common symptoms of asthma include__________ ,coughing,chest tightness,and shortness of breath.
B.Fill in the blanks with the suitable words or expressions from each group.
Bronchiectasis is a disease state defined by localized,irreversible dilation of part of the bronchial tree caused by destruction of the muscle and elastic 1 .It is classified as an obstructive 2 disease,along with emphysema,bronchitis, asthma,and cystic fibrosis.Involved bronchi are dilated,inflamed,and easily collapsible,resulting in airflow 3 and impaired clearance of secretions. Bronchiectasis is associated with a wide range of disorders,but it usually results from 4 infections,such as infections caused by the Staphylococcus or Klebsiella species,or Bordetella pertussis.
In the developed world,immunizations and antibiotics have led to a 5 incidence of this disorder.In these countries,diffuse bronchiectasis is more often found in association with underlying 6 such as immune deficiencies, primary ciliary dyskinesia,and recurrent aspiration syndromes. 7 bronchiectasis is usually associated with bronchial obstruction(i.e.from a foreign body)that leads to infection involving a limited region of the lung.
Bronchiectasis has both congenital and 8 causes,with the latter more frequent.Patients withα1-antitrypsin deficiency have been found to be particularly susceptible to 9 ,for unknown reasons.Other less-common congenital causes include primary immunodeficiencies,due to the weakened or nonexistent 10 system response to severe,recurrent infections that commonly affect the lung.In order to prevent acquired bronchiectasis,children should be immunized against measles,pertussis and other acute 11 infections of childhood.While smoking has not been found to be a direct cause of bronchiectasis,it is certainly an 12 that all patients should avoid in order to prevent the development of infections(such as bronchitis)and further complications.
13 of bronchiectasis includes controlling 14 and bronchial secretions,relieving airway obstructions,and preventing 15 .This includes the prolonged usage of antibiotics to prevent the 16 cycle of infections,as well as eliminating accumulated fluid with postural drainage(体位引流法)and 17 physiotherapy.Regular vaccination against pneumonia,influenza and pertussis are generally 18 .Surgery may also be used to treat localized bronchiectasis,removing obstructions that could cause 19 of the disease.A healthy body mass index(体质指数)and regular doctor visits may have beneficial effects on the 20 of progressing bronchiectasis.
1.A.tissue B.fibrosis C.vessel D.vein
2.A.chronic B.lung C.parenchyma D.tuberculosis
3.A.accumulation B.colonization C.exacerbation D.obstruction
4.A.abdominal B.luminal C.bacterial D.transmissible
5.A.compromising B.ascending C.soaring D.declining
6.A.restorations B.abnormalities C.disorders D.disabilities
7.A.Focal B.Diffuse C.Bronchial D.Purulent
8.A.abnormal B.incidental C.acquired D.epidemic
9.A.bronchiectasis B.airway C.bronchi D.trachea
10.A.circulatory B.respiratory C.invasive D.immune
11.A.intrathoracic B.interior C.extrinsic D.respiratory
12.A.irritant B.symptom C.indication D.obstruction
13.A.Diagnosis B.Treatment C.Determination D.Analysis
14.A.infections B.tumours C.recurrences D.viruses
15.A.impairments B.variation C.complications D.proliferation 16.A.destructive B.continuous C.transient D.extensive
17.A.respiration B.chest C.inspiration D.expiration
18.A.opposed B.advised C.prohibited D.abandoned
19.A.stabilization B.receding C.recession D.progression
20.A.prevention B.restoration C.promotion D.neglect
Ⅲ.Translation
A.Translate the following sentences into Chinese.
1.The bronchial dilatation of bronchiectasis is associated with destructive and inflammatory changes in the walls of airways,often at the level of segmental or subsegmental bronchi.The normal structural components of the wall,including cartilage,muscle,and elastic tissue,are destroyed and may be replaced by fibrous tissue.
2.As protection against infection is compromised,the dilated airways become more susceptible to colonization and growth of bacteria.Thus,a reinforcing cycle can result,with inflammation producing airway damage, impaired clearance of microorganisms,and further infection,which then completes the cycle by inciting more inflammation.
3.Impaired host defense mechanisms are often involved in the predisposition to recurrent infections.The major cause of localized impairment of host defenses is endobronchial obstruction.Bacteria and secretions cannot be cleared adequately from the obstructed airway,which develops recurrent or chronic infection.
B.Translate the following sentences into English.
1.痰液检测常见大量可释放诱发炎性反应介质的中性粒细胞和多种生物体的移位聚生或感染。痰液适度染色和规范培养常可为抗生素治疗提供指导性依据。
2.肺功能检查可显示弥漫性支气管扩张症或伴发慢性阻塞性肺疾病所导致的气流阻塞。气流阻塞的支气管高反应性(hyperreactivity)和一定程度的可逆性(reversibility)较为常见。
Ⅳ.Writing
A.Write an abstract of Text A.
B.Write a topic-related and literature-based report on Bronchiectasis.