Text A Congenital Heart Diseaseinthe Adult
Congenital heart disease(CHD)complicates 1%of all live births in the general population but occurs in 4% of offspring of women with CHD. Substantial numbers of affected infants and children,estimated at>85%currently, reach adulthood because of successful medical and surgical management or because they have successfully adapted to their particular cardiovascular physiology.More than 800,000adults with operated or unoperated CHD exist in the United States today;as such,adults now outnumber children with CHD.
Etiology
CHD is generally the result of aberrant embryonic development of a normal structure or failure of such a structure to progress beyond an early stage of embryonic or fetal development.Malformations are due to complex multifactorial genetic and environmental causes.Recognized chromosomal aberrations and mutations of single genes account for<10%of all cardiac malformations.
The presence of a cardiac malformation as a component of the multiple system involvement in Down syndrome,Turner syndrome,and the trisomy 13-15(D1)and 17-18(E)syndromes may be anticipated in occasional pregnancies by detection of abnormal chromosomes in fetal cells obtained from amniotic fluid or chorionic villus biopsy.Identification in such cells of the enzyme disorders characteristic of Hurler syndrome,homocystinuria,or typeⅡglycogen storage disease may also allow one to predict cardiac disease.
Pathophysiology
The anatomic and physiologic changes in the heart and circulation due to any specific CHD lesion are not static but,rather,progress from prenatal life to adulthood.Malformations that are benign or escape detection in childhood may become clinically significant in the adult.For example,a functionally normal congenitally bicuspid aortic valve may thicken and calcify with time, resulting in significant aortic stenosis;or a well-tolerated left-to-right shunt of an atrial septal defect may result in cardiac decompensation or pulmonary hypertension only after the fourth to fifth decade.
Pulmonary hypertension.The status of the pulmonary vascular bed is often a principal determinant of the clinical manifestations and course of a given lesion and of the feasibility of surgical repair.Increased pulmonary arterial pressure results from increased pulmonary blood flow and/or resistance,the latter is usually the result of obstructive,obliterative structural changes within the pulmonary vascular bed.It is important to quantitate and compare pulmonary to systemic flows and resistances in patients with severe pulmonary hypertension. The causes of pulmonary vascular obstructive disease are unknown,although increased pulmonary blood flow,increased pulmonary arterial blood pressure, elevated pulmonary venous pressure,erythrocytosis,systemic hypoxemia, acidosis,and the bronchial circulation have been implicated.The term“Eisenmenger syndrome”is applied to patients with a large communication between the two circulations at the aortopulmonary,ventricular,or atrial levels and bidirectional or predominantly right-to-left shunts because of high-resistance and obstructive pulmonary hypertension.Pulmonary arterial vasodilators and both single lung transplantation with intracardiac defect repair and total heart-lung transplantation show promise for improvement in symptoms.
Erythrocytosis.Chronic hypoxemia in cyanotic CHD results in secondary erythrocytosis due to increased erythropoietin production.The commonly used term“polycythemia”is a misnomer because white cell counts are normal and platelet counts are normal to decreased.Cyanotic patients with erythrocytosis may have compensated or decompensated hematocrits.Compensated erythrocytosis with iron-replete equilibrium hematocrits rarely results in symptoms of hyperviscosity at hematocrits <65% and occasionally not even with hematocrits<70%.Therapeutic phlebotomy is rarely required in compensated erythrocytosis.In contrast,patients with decompensated erythrocytosis fail to establish equilibrium with unstable,rising hematocrits and recurrent hyperviscosity symptoms.Therapeutic phlebotomy,a two-edged sword,allows temporary relief of symptoms but limits oxygen delivery,begets instability of the hematocrit,and compounds the problem by iron depletion.Iron-deficiency symptoms are usually indistinguishable from those of hyperviscosity;progressive symptoms after recurrent phlebotomy are usually due to iron depletion with hypochromic microcytosis.Iron depletion results in a larger number of smaller(microcytic)hypochromic red cells are less capable of carrying oxygen.Because these microcytes are less deformable in the microcirculation and there are more of them relative to the plasma volume,the viscosity is greater than for an equivalent hematocrit with fewer,larger,iron-replete,deformable cells.As such,iron-depleted erythrocytosis results in increasing symptoms due to decreased oxygen delivery to the tissues.
Hemostasis is abnormal in cyanotic CHD,due in part to the increased blood volume and engorged capillaries,abnormalities in platelet function and sensitivity to aspirin or nonsteroidal anti-inflammatory agents,and abnormalities of the extrinsic and intrinsic coagulation system.Oral contraceptives are often contraindicated for cyanotic women because of the enhanced risk of vascular thrombosis.
The risk of stroke is greatest in children<4 years with cyanotic heart disease and iron deficiency,often with dehydration as an aggravating cause. Adults with cyanotic CHD do not appear to be at increased risk for stroke, unless there are excessive injudicious phlebotomies,inappropriate use of aspirin or anticoagulants,or the presence of atrial arrhythmias or infective endocarditis.
Symptoms of hyperviscosity can be produced in any cyanotic patient with erythrocytosis if dehydration reduces plasma volume.Phlebotomy for symptoms of hyperviscosity not due to dehydration or iron deficiency is a simple outpatient removal of 500 ml of blood over 45 min with isovolumetric replacement with isotonic saline.Acute phlebotomy without volume replacement is contraindicated.Iron repletion in decompensated iron-depleted erythrocytosis reduces iron-deficiency symptoms but must be done gradually to avoid an excessive rise in hematocrit and resultant hyperviscosity.
Pregnancy.The physiologic alterations during normal gestation can create symptoms and physical findings that may be attributed erroneously to heart disease.The mother's health is most at risk if she has a cardiovascular lesion associated with pulmonary vascular disease and pulmonary hypertension(e.g. Eisenmenger physiology or mitral stenosis)or left ventricular(LV)outflow tract obstruction(e.g.aortic stenosis),but she is also at risk of death with any malformation that may cause heart failure or a hemodynamically important arrhythmia.The fetus is most at risk with maternal cyanosis,heart failure,or pulmonary hypertension.Women with aortic coarctation or Marfan syndrome risk aortic dissection.Patients with cyanotic heart disease,pulmonary hypertension, or Marfan syndrome with a dilated aortic root should not become pregnant;those with correctable lesions should be counseled about the risks of pregnancy with an uncorrected malformation versus repair and later pregnancy.The effect of pregnancy in postoperative patients depends on the outcome of the repair, including the presence and severity of residua,sequelae,or complications. Contraception is an important topic with such patients.Tubal ligation should be considered in those in whom pregnancy is strictly contraindicated.
Surgically Modified CHD
Because of the enormous strides in cardiovascular surgical techniques that have occurred in the past 50 years,a large number of long-term survivors of corrective operations in infancy and childhood have reached adulthood.These patients are often challenging because of the diversity of anatomic,hemodynamic, and electrophysiologic residua and sequelae of cardiac operations.
The proper care of the survivor of operation for CHD requires that the clinician understands the details of the malformation before operation;pays meticulous attention to the details of the operative procedure;and recognizes the postoperative residua(conditions left totally or partially uncorrected),the sequelae(conditions caused by surgery),and the complications that may have resulted from the operation.With the exception of ligation and division of an uncomplicated patent ductus arteriosus,almost every other surgical repair of an anomaly leaves behind or causes some abnormality of the heart and circulation that may range from trivial to serious.Intraoperative transesophageal echocardiography assists in detecting unsuspected lesions,in monitoring the repair,and in verifying a satisfactory result or directing further repair.Thus, even with results that are considered clinically to be good to excellent, continued long-term postoperative follow-up is advisable.
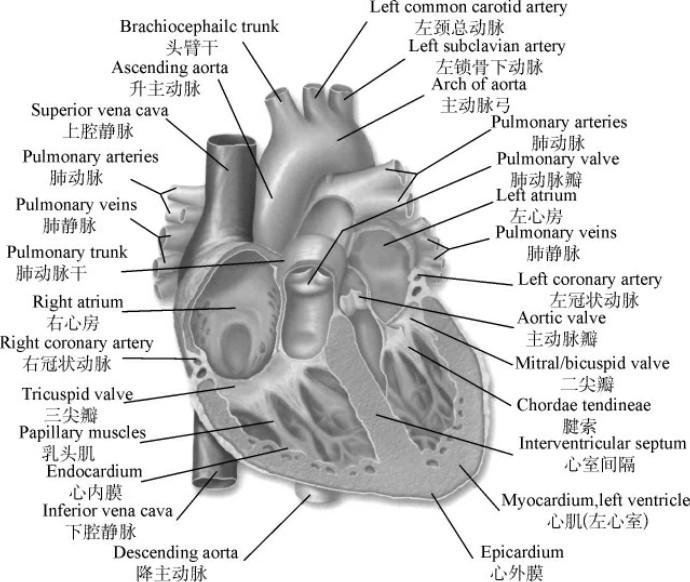
Fig.5-1 Interior of the atrium and ventricle
Cardiac operations importantly involving the atria,such as closure of atrial septal defect,repair of total or partial anomalous pulmonary venous return,or venous switch corrections of complete transposition of the great arteries(the Mustard or Senning operations),may be followed years later by sinus node or atrioventricular node dysfunction or by atrial arrhythmias(especially atrial flutter)(Fig.5-1).Intraventricular surgery may also result in electrophysiologic consequences,including complete heart block necessitating pacemaker insertion to avoid sudden death.In addition,valvular problems may arise late after initial cardiac operation.An example is the progressive stenosis of an initially nonobstructive bicuspid aortic valve in the patient who underwent aortic coarctation repair.Such aortic valves may also be the site of infective endocarditis.After repair of the ostium—primum atrial septal defect,the cleft mitral valve may become progressively regurgitant.Tricuspid regurgitation may also be progressive in the postoperative patient with tetralogy of Fallot if RV outflow tract obstruction was not relieved adequately at initial surgery.In many patients with surgically modified CHD,inadequate relief of an obstructive lesion,or a residual regurgitant lesion,or a residual shunt will cause or hasten the onset of clinical signs and symptoms of myocardial dysfunction. Despite a good hemodynamic repair,many patients with a subaortic right ventricle develop RV decompensation and signs of“left heart failure.”In many patients,particularly those who were cyanotic for many years before operation,apreexisting compromise in ventricular performance is due to the original underlying malformation.
A final category of postoperative problems involves the use of prosthetic valves,patches,or conduits in the operative repair.The special risks include infective endocarditis,thrombus formation,and premature degeneration and calcification of the prosthetic materials.There are many patients in whom extracardiac conduits are required to correct the circulation functionally and often to carry blood to the lungs from the right atrium or right ventricle.These conduits may develop intraluminal obstruction,and,if they include a prosthetic valve,it may show progressive calcification and thickening.
(1,600 words)
New Words and Phrases
aberrant[æ'berənt]a. 异常的
embryonic[,embrɪ'ɒnɪk]a. 胚胎的;未成熟的;未发育好的
multifactorial[,mʌltɪfæk'tɔːrɪəl]a. 多遗传因子的
Down syndrome 唐氏综合征
Turner syndrome 特纳综合征
trisomy['traɪsəʊmɪ]n. 三体性
chorionic[,kɔːrɪ'ɒnɪk]a. 绒(毛)膜的
villus['vɪləs]n. 绒毛;纤毛
enzyme['enzaɪm]n. 酶
Hurler syndrome 赫尔勒综合征
homocystinuria[,həʊməʊ,sɪstɪ'njuːərɪə]n. 高胱氨酸尿症
glycogen storage disease 糖原储积症
septal['septəm]([复]septa)a. 隔膜的;间隔的
decompensation[diː,kɒmpən'seɪʃən]n. 代偿失调
acidosis[,æsɪ'dəʊsɪs]n. 酸中毒
Eisenmenger syndrome 艾森门格综合征
erythrocytosis[ɪ,rɪθrəʊsaɪ'təʊsɪs]n. 红细胞增多(症)
hypoxemia[,haɪpɔːk'siːmɪə]n. 低氧血(症)
cyanotic[,saɪə'nɔːtɪk]a. 发绀的
erythropoietin[ɪ,rɪθrəʊ'pɒɪətɪn]n. 红细胞生成素
polycythemia[,pɒlɪsaɪ'θiːmɪə]n. 红细胞增多症
hematocrit['hemətəʊkrɪt,hɪ'mætəkrɪt]n. 血细胞比容
equilibrium[,iːkwɪ'lɪbrɪəm]n. 均衡
hyperviscosity[,haɪpзːvɪs'kɒsɪtɪ]n. 黏滞性过高
phlebotomy[flɪ'bɒtəmɪ]n. 放血
recurrent[rɪ'kʌrənt]a. 周期性的;复发的
hypochromia[,haɪpə'krəʊmɪə]n. 血红蛋白过少
microcytosis[,maɪkrəʊsaɪ'təʊsɪs]n. 小红细胞症
viscosity[vɪ'skɒsətɪ]n. 黏性;黏度
hemostasis[,hɪmɒʊ'steɪsɪs]n. 止血;止血法
nonsteroidal[,nɒnstə'rɒɪdəl]a. 非类固醇的
anti-inflammatory[,æntɪɪn'flæmətərɪ]n. 消炎药
contraindicate[,kɒntrə'ɪndɪkeɪt]v. 禁忌(某种疗法、药物等)
thrombosis[θrɒm'bəʊsɪs]n. 血栓形成
dehydration[,diːhaɪ'dreɪʃən]n. 脱水
anticoagulant[,æntɪkəʊ'æɡjʊlənt]n. 抗凝血药
arrhythmia[ə'rɪðmɪə]n. 心律失常
endocarditis[,endəʊkɑː'daɪtɪs]n. 心内膜炎
isovolumetric[,aɪsəʊ,vɒljʊ'metrɪk]a. 等容的
isotonic[,aɪsəʊ'tɒnɪk]a. 等渗的;等压的
mitral['maɪtrəl]a. 二尖瓣的
mitral stenosis['maɪtrəl stɪ'nəʊsɪs] 二尖瓣狭窄
fetus['fiːtəs]n. 胎儿
coarctation[,kəʊaːk'teɪʃən]n. 缩窄
aortic coarctation 主动脉缩窄
Marfan syndrome 马方综合征
aortic dissection[eɪ'ɔːtɪk dɪ'sekʃən] 主动脉夹层
residuum[rɪ'zɪdjʊəm]([复]residua)n. 残渣;残余
sequela[sɪ'kwiːlə]([复]sequelae)n. 后遗症
contraception[,kɒntrə'sepʃən]n. 避孕
tubal['tjuːbəl]a. 输卵管的
ligation[laɪ'ɡeɪʃən]n. 结扎
arteriosus[,ɑːtɪərɪ'əʊsəs]a. 动脉的
transesophageal[transiː,sɒfə'dʒiːəl]a. 经食管的
atrium['ɑːtrɪəm]([复]atria)n. 心房
sinus['saɪnəs]n. 窦
node[nəʊd]n. 结,结节
atrioventricular[,eɪtrɪəʊven'trɪkjʊlə]a. 心房与心室的,房室的
pacemaker['peɪs,meɪkə]n. (心脏)起搏器
tricuspid[traɪ'kʌspɪd]a. 三尖瓣的
tetralogy of Fallot 法洛四联症
ventricle['ventrɪkl]n. 心室
thrombus['θrɒmbəs]n. 血栓
calcification[,kælsɪfɪ'keɪʃən]n. 钙化
intraluminal[,ɪntrə'luːmɪnəl]a. 管腔内的
 Exercises
Exercises
Ⅰ.Reading Comprehension
A.Answer the following questions.
1.What causes can result in congenital heart disease(CHD)?
2.What symptoms will be implicated in pulmonary vascular obstruction disease?
3.How do we describe the patients with Eisenmenger syndrome?
4.What is the result of iron-deficiency symptoms caused by therapeutic phlebotomy?
5.Is there any valvular problem late after initial cardiac operation?Give one or two examples.
B.Choose the right answer to each question.
1.Which of the following statements about hemostasis in cyanotic CHD is NOT true?
A.The increased blood volume and engorged capillaries.
B.Abnormalities in platelet function.
C.Sensitivity to aspirin or steroidal anti-inflammatory agents.
D.Abnormalities of the extrinsic and intrinsic coagulation system.
2.__________ may not make adults with cyanotic CHD appear to be at increased risk for stroke.
A.Restrained phlebotomies
B.Inappropriate use of aspirin or anticoagulants
C.The presence of atrial arrhythmias
D.The presence of infective endocarditis
3.A mother with cardiovascular lesion,pulmonary hypertension and left ventricular(LV)outflow tract obstruction will make her health__________at risk.
A.never B.less C.fewer D.most
4.The anatomic and physiologic changes in the heart and circulation due to any specific CHD lesion are not static but,rather,progress from__________to__________ .
A.prenatal life;childhood B.prenatal life;adulthood
C.childhood;the elderly D.childhood;adulthood
5.According to the passage,which of the following statements is NOT true?
A.Cyanotic patients with erythrocytosis may have compensated or decompensated hematocrits.
B.The fetus is most at risk with maternal cyanosis,heart failure,or pulmonary hypertension.
C.Despite a good hemodynamic repair,many patients with a subaortic right ventricle develop RV decompensation and signs of“left heart failure”.
D.These conduits may develop intraluminal obstruction,and,if they include a prosthetic valve,it may show progressive calcification and thinning.
Ⅱ.Words and Expressions
A.Fill the blanks with the words or expressions given below,and change the form where necessary.
cyanotic hematocrit ligation cardiac decompensation
ventricle congenital thrombus arrhythmia chromosome
erythrocytosis phlebotomy stenosis hemostasis atria
1.__________ heart disease occurs when the heart is malformed before birth, and is the most common of all birth defects.
2.The blood requirements should be determined by the__________ .
3.If the Y__________ is detected,the fetus is male.
4.As a simple and effective medical treatment,venesection and__________ therapy could be the supplement of other therapy and method of adjunctive therapy.
5.Aortic__________ is the inability of the aortic valve to open completely.
6.When to see the wound bleeding,most often done by hand by holding down the emergency action is bleeding area,which is oppression__________ .
7.Cerebral abscess is a serious condition and in children the commonest cause is__________ congenital heart disease.
8.He died of severe exhaustion and dehydration that lead to__________ arrest or heart failure.
9.This patient developed severe hepatitis with hepatic__________ .
10.Both__________ are thin walled muscular chambers.
B.Fill in the blanks with the suitable words or expressions from each group.
In unaffected individuals,the chambers of the left side of the heart are under higher pressure than the chambers of the right side of the heart.This is because the 1 has to produce enough pressure to pump blood throughout the entire body,while the right ventricle only has to produce enough pressure to pump blood to the 2 .
In the case of a large ASD(diameter>9 mm),which may result in a clinically remarkable 3 shunt,blood will shunt from the left atrium to the right atrium.This extra blood from the left atrium may cause a volume 4 of both the right atrium and the right ventricle.If untreated,this condition can result in 5 of the right side of the heart and ultimately 6 .
Any process that increases the pressure in the left ventricle can cause worsening of the left-to-right shunt.This includes 7 ,which increases the pressure that the left ventricle has to generate in order to open the 8 valve during 9 systole,and coronary artery disease which increases the stiffness of the left ventricle,thereby increasing the filling pressure of the left ventricle during 10 diastole.
The right ventricle will have to push out more blood than the left ventricle due to the left-to-right shunt.This constant overload of the right side of the heart will cause an overload of the entire pulmonary vasculature.Eventually 11 hypertension may develop,which will cause the right ventricle to face increased 12 in addition to the increased preload that the shunted blood from the left atrium to the right atrium caused.The right ventricle will be forced to generate higher pressures to try to overcome the pulmonary hypertension.This may lead to 13 (dilatation and decreased systolic function of the right ventricle).
When the pressure in the right atrium 14 to the level in the left atrium,there will no longer be a pressure gradient between these heart 15 , and the left-to-right shunt will diminish or cease.
If left uncorrected,the pressure in the right side of the heart will be 16 than the left side of the heart.This will cause the pressure in the right atrium to be higher than the pressure in the left atrium.This will reverse the pressure gradient across the ASD,and the 17 will reverse;a right-to-left shunt will exist.This phenomenon is known as 18 .
Once right-to-left shunting occurs,aportion of the 19 blood will get shunted to the left side of the heart and ejected to the peripheral vascular system.This will cause signs of 20 .
1.A.right ventricle B.left ventricle C.left atrium D.right atrium
2.A.chambers B.heart C.lungs D.brain
3.A.bidirectional B.left-to-right C.right-to-left D.systemic-to-pulmonary
4.A.expand B.decline C.underload D.overload
5.A.shrinkage B.contraction C.enlargement D.wideness
6.A.ventricular septal defect B.atrial septal defect C.congenital heart defects D.heart failure
7.A.hypertension B.erythrocytosis C.aortic stenosis D.polycythemia
8.A.tricuspid B.aortic C.mitral D.pulmonary
9.A.atrial B.ventricular C.electrical D.mechanical
10.A.ventricular B.atrial C.mechanical D.electrical
11.A.arterial B.secondary C.pulmonary D.primary
12.A.afterload B.preload C.blood pressure D.aortic pressure
13.A.chronic heart failure B.biventricular failure C.myocardial infarction D.right ventricular failure
14.A.rises B.increases C.declines D.decreases
15.A.ventricle B.myocardium C.atrium D.chambers
16.A.harder B.less C.greater D.weaker
17.A.circulatory system B.pulmonary vasculature C.blood flow D.shunt
18.A.Turner syndrome B.Down syndrome C.Eisenmenger syndrome D.tetralogy of Fallot
19.A.oxygenated B.oxygen-carrying C.oxygen-depleted D.oxygen-poor
20.A.acropachy B.cyanosis C.hemothorax D.hemoptysis
Ⅲ.Translation
A.Translate the following sentences into Chinese.
1.CHD is generally the result of aberrant embryonic development of a normal structure or failure of such a structure to progress beyond an early stage of embryonic or fetal development.Malformations are due to complex multifactorial genetic and environmental causes.Recognized chromosomal aberrations and mutations of single genes account for<10%of all cardiac malformations.
2.The presence of a cardiac malformation as a component of the multiple system involvement in Down syndrome,Turner syndrome,and the trisomy 13-15(D1)and 17-18(E)syndromes may be anticipated in occasional pregnancies by detection of abnormal chromosomes in fetal cells obtained from amniotic fluid or chorionic villus biopsy.
3.For example,a functionally normal congenitally bicuspid aortic valve may thicken and calcify with time,resulting in significant aortic stenosis;or a well-tolerated left-to-right shunt of an atrial septal defect may result in cardiac decompensation or pulmonary hypertension only after the fourth to fifth decade.
B.Translate the following sentences into English.
1.先天性心脏病的发病率在新生儿(neonate)中高达6.7‰,每年我国有15万~20万例先天性心脏病新生儿出生。如果不给予任何治疗,其中1/3新生患儿将因病情严重在出生后6~12个月内死亡。
2.心律失常是危重先天性心脏病婴幼患儿术后主要的并发症之一。心律失常的准确诊断和及时治疗可以有效地降低危重先天性心脏病婴幼患儿心脏手术的死亡率。
Ⅳ.Writing
A.Write an abstract of Text A.
B.Write a topic-related and literature-based report on Acquired Heart Disease.