Text A Diabetes Mellitus
Diabetes mellitus(DM),often simply referred to as diabetes,is a group of metabolic diseases in which a person has high blood sugar,either because the body does not produce enough insulin,or because cells do not respond to the insulin that is produced(Fig.4-1).This high blood sugar produces the classical symptoms of polyuria(frequent urination),polydipsia(increased thirst)and polyphagia(increased hunger)(Fig.4-2).
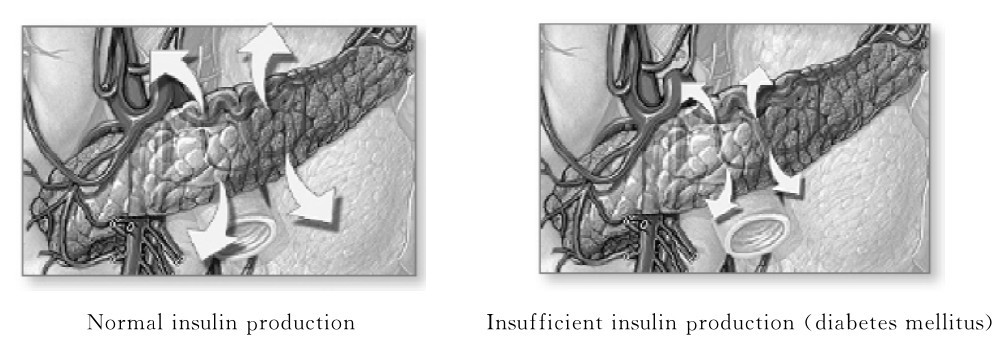
Fig.4-1 Contrast between normal insulin production and insufficient insulin production
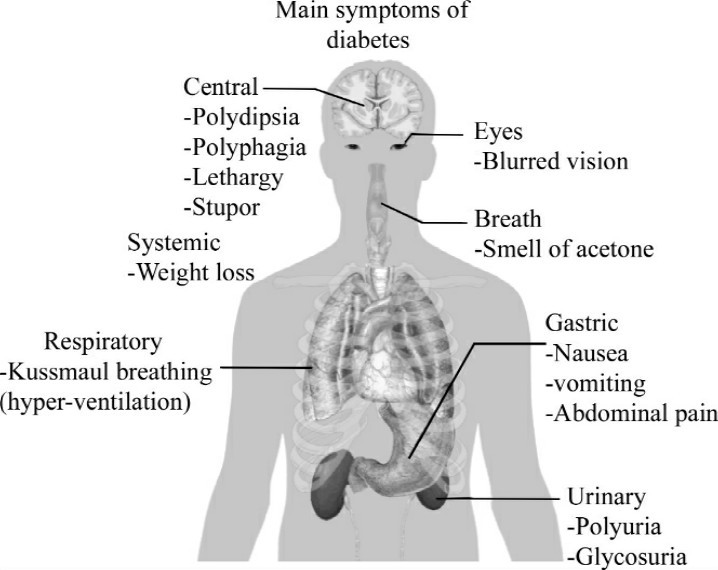
Fig.4-2 Symptoms of diabetes showed in the whole body
Type 1:Insulin-dependent Diabetes Mellitus(IDDM)
IDDM is characterized by little or no endogenous insulin secretion.Because of the marked hypoinsulinemia,patients with this disorder usually present with the acute complications of diabetes mellitus such as polyuria,polydipsia, polyphagia,and ketoacidosis.In order to prevent ketoacidosis and death,these patients require exogenous insulin replacement.After the onset of diabetes, patients occasionally enter a“honeymoon phase”that may last several weeks or months during which time endogenous insulin secretion is restored and glucose metabolism may approach normal.Unfortunately,the disease invariably relapses and lifelong insulin therapy is required.
The peak age of onset of IDDM is between 11 and 13 years,coinciding with the onset of puberty,but IDDM can begin at any age,including the elderly.Patients with this disorder are usually of normal weight or thin. Specific human leucocyte antigen(HLA)phenotypes occur at a much greater frequency in patients with IDDM than in the general population.There is less than a 50%concordance rate for diabetes in identical twins with IDDM(i.e. less than50%of identical twins both have diabetes),suggesting the importance of both genetic and environmental factors.
The etiology of IDDM is unknown.A leading hypothesis is that a viral illness or another yet unspecified initiating event may damage the beta cells of the pancreas,followed by a slow autoimmune destruction of the remaining beta cells in susceptible individuals.Anti-islet cell and anti-insulin antibodies may be detected in individuals several years prior to the onset of diabetes,followed by a slow deterioration in glucose tolerance which finally results in the abrupt onset of clinical diabetes.Soon after the onset of the disease,antibodies against the islet cells of the pancreas are present in as high as 90%of patients with IDDM,but they diminish in frequency to 5%to 10%after 20 years.This autoimmune hypothesis would also account for the increased risk of developing diabetes in individuals with certain HLA genes,because the genes that control the immune response are located on the sixth chromosome close to the HLA genes loci.
The goal of therapy for this disease is to design and implement insulin regimens that mimic physiologic insulin secretion.Because individuals with IDDM partially or completely lack endogenous insulin production,administration of basal,exogenous insulin is essential for regulating glycogen breakdown, gluconeogenesis,lipolysis,and ketogenesis.Likewise,insulin replacement for meals should be appropriate for the carbohydrate intake and promote normal glucose utilization and storage.
Nowadays,whole pancreas transplantation(performed concomitantly with a renal transplant)may normalize glucose tolerance and is an important therapeutic option in IDDM,though it requires substantial expertise and is associated with the side effects of immunosuppression.Pancreatic islet transplantation has been plagued by limitations in pancreatic islet isolation and graft survival and remains an area of clinical investigation.Many individuals with long-standing IDDM still produce very small amounts of insulin or have insulin-positive cells within the pancreas.This suggests that beta cells are slowly regenerating but are quickly destroyed by the autoimmune process.Thus, efforts to suppress the autoimmune process and to stimulate beta cell regeneration are underway both at the time of diagnosis and in years after the diagnosis of IDDM.Closed-loop pumps that infuse the appropriate amount of insulin in response to changing glucose levels are potentially feasible now that continuous glucose-monitoring technology has been developed.
Type 2:Non-insulin-dependent Diabetes Mellitus(NIDDM)
NIDDM is much more common than IDDM(about 90%of cases of diabetes)and usually has its onset after age 30.Obesity is the primary cause of NIDDM in people who are genetically predisposed to the disease.It is a metabolic disorder with high blood glucose in the context of insulin resistance combined with relative reduced insulin secretion.The classic symptoms are polydipsia,polyuria and constant hunger.
Plasma insulin levels are relatively decreased in patients with NIDDM but are not as severely reduced as in IDDM.Because insulin deficiency is not marked,ketoacidosis rarely occurs in NIDDM unless a stressful event such as a myocardial infarction or infection is superimposed.
In addition to the abnormalities of insulin secretion,patients with NIDDM are also resistant to the action of insulin.This insulin resistance is due both to a decrease in insulin binding to its plasma membrane receptor and to postreceptor defects in insulin action.Thus,both a decrease in insulin secretion and impaired insulin action contribute to the hyperglycemia observed in NIDDM. At this time,the relative importance of these abnormalities in producing the impaired glucose metabolism is unclear.
The goals of therapy for NIDDM are similar to those in IDDM.While glycemic control tends to dominate the management of IDDM,the care of individuals with NIDDM must also include attention to the treatment of conditions associated with NIDDM (obesity,hypertension,dyslipidemia, cardiovascular disease)and detection/management of diabetes mellitus-related complications.Diabetes mellitus-specific complications may be present in up to 20%—50% of individuals with newly diagnosed NIDDM.Reduction in cardiovascular risk is of paramount importance as this is the leading cause of mortality in these individuals.Efforts to achieve blood pressure and lipid goals should begin in concert with glucose-lowering interventions.
NIDDM management should begin with medical nutrition therapy.An exercise regimen to increase insulin sensitivity and promote weight loss should also be instituted.Pharmacologic approaches to the management of NIDDM include oral glucose-lowering agents,insulin,and other agents that improve glucose control;most physicians and patients prefer oral glucose-lowering agents as the initial choice.Any therapy that improves glycemic control reduces“glucose toxicity”to the islet cells and improves endogenous insulin secretion.However, NIDDM is a progressive disorder and ultimately requires multiple therapeutic agents and often insulin.
Insulin should be considered as the initial therapy in NIDDM,particularly in lean individuals or those with severe weight loss,in individuals with underlying renal or hepatic disease that precludes oral glucose-lowering agents,or in individuals who are hospitalized or acutely ill.Insulin therapy is ultimately required by a substantial number of individuals with NIDDM because of the progressive nature of the disorder and the relative insulin deficiency that develops in patients with long-standing diabetes.Both physician and patient reluctance often delay the initiation of insulin therapy,but glucose control and patient well-being are improved by insulin therapy in patients who have not reached the glycemic target.
(1,114 words)
New Words and Phrases
diabetes[,daɪə'biːtiːz]n. 糖尿病
metabolic[,metə'bɒlɪk]a. 新陈代谢的
insulin['ɪnsjʊlɪn]n. 胰岛素
polydipsia[,pɒlɪ'dɪpsɪə]n. 烦渴
polyphagia[,pɒlɪ'feɪdʒɪə]n. 贪食(症),食欲过盛
endogenous[en,dɒdʒənəs]a. 内源的,内生的
hypoinsulinemia[,haɪpəʊ,ɪnsəlɪ'niːmɪə]n. 低胰岛素血症
ketoacidosis[,kiːtəʊ,æsɪ'dəʊsɪs]n. 酮症酸中毒
exogenous[ek'sɒdʒənəs]a. 外源的,外生的
glucose['ɡluː,kəʊs]n. 葡萄糖
puberty['pjuːbətɪ]n. 青春期;发育
phenotype['fiːnəʊtaɪp]n. 表型
concordance[kən'kɔːdəns]n. 一致,符合;(发病)一致性
beta cell β细胞
pancreas['pæŋkrɪəs]n. 胰腺
islet['aɪlɪt]n. 胰岛
anti-islet 抗胰岛
chromosome['krəʊməsəʊm]n. 染色体
locus['ləʊkəs]([复]loci)n. 位点,部位
gluconeogenesis['ɡluːkəʊ,niːəʊ'dʒenɪsɪs]n. 糖原异生(作用)
lipolysis[lɪ'pɒlɪsɪs]n. 脂解(作用)
ketogenesis[,kiːtəʊ,dʒenɪsɪs]n. 生酮作用
immunosuppression[,ɪmjʊnəʊsə'preʃən]n. 免疫抑制
pancreatic[,pæŋkrɪ'ætɪk]a. 胰腺的
pancreatic islet 胰岛
superimpose[,sjuːpərɪm'pəʊz]v. 添加,附加
impair[ɪm'peə]v. 损害,削弱
glycemic[ɡlaɪ'siːmɪk]a. 血糖的
hypertension[,haɪpə'tenʃən]n. 高血压
dyslipidemia[dɪs,lɪpɪ'dɪmɪə]n. 血脂异常
toxicity[tɒk'sɪsətɪ]n. 毒性,毒力
hepatic[hɪ'pætɪk]a. 肝脏的
 Exercises
Exercises
Ⅰ.Reading Comprehension
A.Answer the following questions.
1.What is diabetes mellitus?
2.What complications do patients with type 1 diabetes present with?
3.What is a leading hypothesis of the etiology of IDDM?
4.Why are patients with NIDDM resistant to the action of insulin?
5.What are the goals of therapy for NIDDM?
B.Decide whether the following statements are True or False.
1.Specific HLA phenotypes occur at a much low frequency in patients with IDDM than in the general population.
2.Because individuals with IDDM partially or completely lack endogenous insulin production,administration of basal,exogenous insulin is essential for regulating glycogen breakdown,gluconeogenesis,lipolysis,and ketogenesis.
3.Efforts to suppress the autoimmune process and to stimulate beta cell regeneration are underway both at the time of diagnosis and in years after the diagnosis of IDDM.
4.Plasma insulin levels are relatively decreased in patients with NIDDM but are as severely reduced as in IDDM.
5.Pharmacologic approaches to the management of NIDDM include oral glucose-lowering agents,insulin,and other agents that improve glucose control.
Ⅱ.Words and Expressions
A.Fill in the blanks with the words or expressions given below,and change the form where necessary.
polydipsia lipolysis endogenous insulin ketoacidosis
exogenous ketogenesis carbohydrate glucose renal
pancreatic hypertension cardiovascular glycemic gluconeogenesis
1.Because individuals with IDDM partially or completely lack endogenous insulin production,administration of basal,__________ insulin is essential for regulating glycogen breakdown,gluconeogenesis,lipolysis and ketogenesis.
2.Insulin replacement for meals should be appropriate for the__________ intake and promote normal glucose utilization and storage.
3.The benefits of intensive diabetes management and improved__________ control include a reduction in the microvascular complications of diabetes mellitus and a reduction in the macrovascular complications of diabetes mellitus.
4.A shortcoming of current insulin regimens is that injected insulin immediately enters the systemic circulation,whereas__________ insulin is secreted into the portal venous system.
5.Insulin infusion devices present unique challenges,such as infection at the infusion site,unexplained hyperglycemia because the infusion set becomes obstructed,or diabetic__________ if the pump becomes disconnected.
6.Pharmacologic approaches to the management of NIDDM include oral glucose-lowering agents,__________ ,and other agents that improve glucose control.
7.Hypoglycemia is usually related to delayed meals,increased physical activity,alcohol intake,or__________ insufficiency.
8.NIDDM may have associated conditions such as insulin resistance,__________ , cardiovascular disease,dyslipidemia or polycystic ovary syndrome.
9.Individuals at high risk for__________ disease should be screened by appropriate cardiac stress testing.
10.Insulin released from__________ beta cell at a low basal rate and at a much higher stimulated rate in response to a variety of stimuli,especially glucose.
B.Fill in the blanks with the suitable words or expressions from each group.
Diabetes is a serious disease.Following your diabetes treatment plan takes round-the-clock commitment.But your efforts are 1 .Careful diabetes care can reduce your risk of serious—even life-threatening—complications.
Members of your diabetes care team—doctor,diabetes nurse educator and dietitian,for example—will help you learn the basics of diabetes care and offer 2 and encouragement along the way.But it's 3 to you to manage your condition.After all,no one has a greater stake in your health than you. Learn all you can about diabetes.Make healthy eating and 4 activity part of your daily routine. 5 a healthy weight.Monitor your blood sugar level, and follow your doctor's 6 for keeping your blood 7 level within your target range.Don't be afraid to ask your diabetes treatment team for help when you need it.
If you smoke or use other types of tobacco,ask your doctor to help you 8 .Smoking increases your risk of various diabetes 9 ,including heart attack,stroke,nerve damage and kidney disease.In fact,smokers who have 10 are three times more likely to die of cardiovascular disease than are nonsmokers who have diabetes,according to the American Diabetes Association.Talk to your doctor about ways to stop smoking or to stop using other types of tobacco.
Like diabetes,high blood pressure can damage your blood 11 .High cholesterol is a concern,too,since the damage is often worse and more rapid when you have diabetes.When these conditions team up,they can lead to a heart 12 ,stroke or other life-threatening conditions.Eating 13 foods and exercising regularly can go a long way toward controlling high blood pressure and 14 .Sometimes medication is needed,too.
Diabetes may leave you prone to gum infections.Brush your teeth at least twice a day,floss your teeth once a day,and schedule 15 exams at least twice a year.Consult your dentist right away if your gums bleed or look red or 16 .
Aspirin reduce your blood's ability to clot.Taking a daily 17 can reduce your risk of heart attack and stroke—major concerns when you have diabetes.In fact,daily aspirin therapy is recommended for most people who have diabetes.Ask your doctor about daily aspirin 18 ,including which strength of aspirin would be best.
If you are stressed,it's easy to neglect your usual diabetes care routine. The hormones your body may produce in response to prolonged stress may prevent 19 from working properly,which only makes matters worse.To take control,set limits.Prioritize your tasks.Learn relaxation techniques.Get plenty of sleep.
Above all,stay positive.Diabetes care is within your control.If you are willing to do your part, 20 won't stand in the way of an active,healthy life.
1.A.worthwhile B.fruitless C.joint D.previous
2.A.occupation B.complaint C.support D.history
3.A.decided B.up C.apt D.alert
4.A.physical B.mental C.emotional D.psychological
5.A.Put B.Use C.Place D.Maintain
6.A.medicines B.examinations C.instructions D.signs
7.A.sugar B.pressure C.bleeding D.circulation
8.A.keep B.smoke C.quit D.take
9.A.complications B.symptoms C.illnesses D.syndromes
10.A.diabetes B.complaints C.infection D.chills
11.A.joints B.vessels C.muscles D.bleeding
12.A.disease B.circulation C.attack D.blood
13.A.healthy B.infected C.delicious D.sweet
14.A.stress B.cholesterol C.hypotension D.depression
15.A.dental B.lip C.mouth D.skeletal
16.A.swollen B.inflammatory C.painful D.pale
17.A.aspirin B.vitamin C.calorie D.fat
18.A.medication B.medicine C.therapy D.care
19.A.diabetes B.insulin C.sugar D.body
20.A.diabetes B.hypertension C.hypotension D.hypoinsulinemia
Ⅲ.Translation
A.Translate the following sentences into Chinese.
1.IDDM is characterized by little or no endogenous insulin secretion.Because of the marked hypoinsulinemia,patients with this disorder usually present with the acute complications of diabetes mellitus such as polyuria, polydipsia,polyphagia,and ketoacidosis.In order to prevent ketoacidosis and death,these patients require exogenous insulin replacement.
2.The goal of therapy for this disease is to design and implement insulin regimens that mimic physiologic insulin secretion.Because individuals with IDDM partially or completely lack endogenous insulin production, administration of basal,exogenous insulin is essential for regulating glycogen breakdown,gluconeogenesis,lipolysis,and ketogenesis.
3.In addition to the abnormalities of insulin secretion,patients with NIDDM are also resistant to the action of insulin.This insulin resistance is due both to a decrease in insulin binding to its plasma membrane receptor and to postreceptor defects in insulin action.Thus,both a decrease in insulin secretion and impaired insulin action contribute to the hyperglycemia observed in NIDDM.
B.Translate the following sentences into English.
1.糖尿病的临床特点是高血糖,可出现多尿、多饮、食欲过盛等症状。一旦血糖得不到有效控制,就会引发并发症,导致肾、眼、足部位的病变,且无法治愈。
2.2型糖尿病的发病与遗传和环境的相关性更为显著。目前公认的病因是胰岛素抵抗和胰岛素分泌不足并存。有些2型糖尿病的病因以胰岛素抵抗为主,伴有胰岛素分泌不足;有些则是胰岛素不足伴有或不伴有胰岛素抵抗。
Ⅳ.Writing
A.Write an abstract of Text A.
B.Write a literature-based and topic-related report on Diabetes Mellitus and Pregnancy.