Text A Primary Malignant Bone Tumors
Primary bone malignancies are relatively uncommon tumors that arise from cells that are normal components of bone tissues and that have the potential to metastasize.Malignant tumors are to be distinguished from a variety of more common benign bone lesions,such as osteochondromas and enchondromas.
Patients with primary malignant and benign bone tumors present with pain,swelling and occasionally pathologic fracture of the involved bone.If radiologic studies suggest a malignant primary bone tumor,an orthopedic oncologist should be consulted before carrying out a biopsy because improper biopsy technique may compromise subsequent surgical care,particularly limb-sparing surgery.Staging of patients with bone tumors generally requires computed tomography(CT)scans of the chest,abdomen,and pelvis to assess for metastatic disease.Characterization of the primary bone tumor may benefit from magnetic resonance imaging(MRI)assessment of soft tissue extension or CT scan assessment of cortical bone involvement,or both.
Osteosarcoma
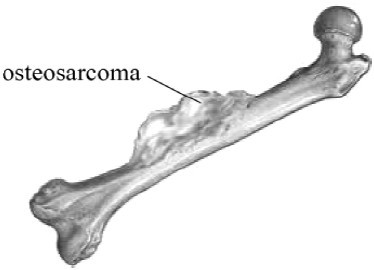
Fig.3-1 Osteosarcoma
Osteosarcoma(Fig.3-1)is the most common malignant sarcoma of bone,representing about 35%of the cases.It has a bimodal age distribution, with highest incidence in patients younger than 20 years,most likely related to the normal rapid bone growth that occurs during adolescence.In this age group,most tumors arise in the metaphyseal areas of the long bones of the extremities,particularly around the knee.Males are affected more commonly than females at a ratio of 3∶2.A second peak of incidence occurs in adults older than 60 years.The site of origin in these older patients are somewhat more heterogeneous,with craniofacial and pelvic bones each accounting for 20%of tumors.Radiographically,osteosarcomas usually present as mixed osteoblastic and osteolytic lesions,although pure forms of either appearance can occur.Periosteal elevation(Codman's triangle),cortical destruction,and tumor extension into soft tissue are common on plain films or MRI.
The incidence of osteosarcoma is increased in families that carry germline deletion of retinoblastoma(Rb),p53(Li-Fraumeni),or Rec Q DNA helicase (Rothman-Thompson,Werner,or Bloom syndrome)genes.Consistent with these observation,although most younger patients with osteosarcomas have no apparent predisposing factor or family history of bone tumors,alterations in the p53 and Rb genes of such sporadic tumors occur in 40% and 60%respectively.In older patients,a variety of conditions may predispose patients to osteosarcoma,most convincingly antecedent Paget's disease or prior radiation therapy.
Osteosarcoma is a highly proliferative neoplasm that metastasizes rapidly. As for most sarcomas,osteosarcoma spreads hematogenously,and the most common site of metastasis is the lung.Despite aggressive surgical resection of the primary bone tumor,the incidence of recurrence with metastatic disease is high in the absence of systemic treatment,consistent with the concept that most patients present with clinically inapparent micrometastatic disease.The development of effective systemic chemotherapy with doxorubicin and cisplatin,with or without methotrexate,has had a profoundly positive effect on treatment outcome,with5-year disease-free survival rates exceeding 65%in patients younger than 40 years with non-metastatic extremity tumors.Most patients are managed with initial neoadjuvant chemotherapy,delayed resection of the primary tumor,and then further postoperative chemotherapy.Serum alkaline phosphatase levels,often elevated in osteosarcoma patients,can be used to monitor disease status.
Modern surgical techniques have allowed surgical resection of most extremity osteosarcomas without amputation.Although resection of lung metastases can be curative in about 20%of selected patients,detection of radiologically apparent metastatic disease at presentation significantly worsens prognosis.Long-term disease control in older adults with osteosarcoma is substantially lower than in younger patients,with a 5-year overall survival rate of 22%in one series of patients older than 65 years,most likely because of fundamental differences in the underlying molecular pathophysiology of tumors in older adults.Although osteosarcoma is generally considered to be relatively radiation resistant,radiation can play apalliative role in selected patients.
Chondrosarcoma
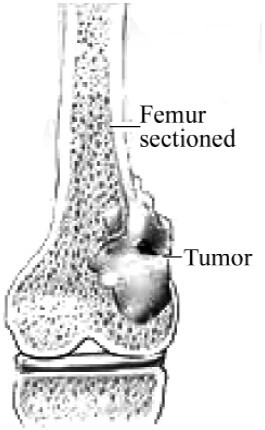
Fig.3-2 Chondrosarcoma
Chondrosarcoma(Fig.3-2),a malignant tumor characterized by hyaline cartilage differentiation,is the second most common sarcoma of bone,representing 25%of bone sarcomas.The peak incidence is in the fifth to seventh decades of life.The most common primary sites are in the pelvis,proximal femur,and proximal humerus.Patients present with long-standing complaints of swelling,pain,or both. Radiographically,chondrosarcoma is detected as an area of radiolucency with variable punctate mineralization,with frequent cortical bone erosion or thickening,sometimes with extension into adjacent soft tissue.Distinguishing low-grade chondrosarcomas from benign central enchondromas can be difficult:location in the axial skeleton and size greater than 5 cm favor malignancy.
Up to15%of chondrosarcomas arise from preexisting peripheral osteochondromas and,like their benign counterparts,harbor mutations in the exostosin(EXT) genes.The remaining 85%of chondrosarcomas arise in a central location,some in preexisting enchondromas.Chondrosarcomas are divided into three grades, with higher-grade tumors characterized by greater cellularity and cellular atypia.In one series,61%of patients had grade 1 tumors;only 4%of such patients developed metastases.In contrast,36%of patients had grade 2 and3%had grade 3 tumors;among this combined group,29%developed matastases.
Unlike osteosarcoma and Ewing's sarcoma,chondrosarcoma generally grow slowly,metastasize less commonly,and have an excellent prognosis after adequate surgical resection.Although chondrosarcomas are considered relatively radiation resistant,radiation therapy may provide palliation for patients with large or recurrent unresectable central chondrosarcomas.
Ewing's Sarcoma
Ewing's sarcoma and primitive neuroectodermal tumor(PNET)are a family of small round cell sarcomas that represent 16%of primary bone sarcomas.As with osteosarcoma,the peak incidence occurs during the second decade of life,but unlike osteosarcoma,the incidence of Ewing's sarcoma is unimodal,being distinctly unusual in older adults and in nonwhites.Ewing's sarcoma tends to arise in the diaphyseal region of long bones,in the pelvis,or in ribs.Ewing's tumors are characterized radiologically by apermeative or“moth-eaten”appearance of the affected bone,with a multilayered“onion-skin”periosteal reaction.MRI studies frequently document a significant soft tissue mass associated with the bone lesion.Unlike other sarcomas of bone, Ewing's sarcoma may present with symptoms of an inflammatory systemic illness,with intermittent fevers,anemia,leukocytosis,and an increased sedimentation rate.Because Ewing's sarcoma resembles other small round cell tumors microscopically,reverse transcription-polymerase chain reaction(RT-PCR)and fluorescent in situ hybridization studies that document such translocations play a critical role in confirming the diagnosis.
The development of effective systemic chemotherapy regimens has substantially improved long-term control of Ewing's sarcoma.After completion of staging procedures,patients are treated with neoadjuvant chemotherapy. After 3 months of chemotherapy,the primary tumor is resected,radiated,or both,depending on the location and extent of the primary tumor. Chemotherapy is then resumed for a total of up to 1 year of treatment.Using such an approach,the mean 5-year event-free survival rate for patients who present with non-metastatic disease is 69%.Insulin-like growth factor-1 receptor antagonists have demonstrated clinical activity in recent clinical trials for chemotherapy-refractory disease.
(1,133 words)
New Words and Phrases
primary['praɪmərɪ]a. 原发的
malignant[mə'lɪɡnənt]a. 恶性的;致命的
metastasize[mə'tæstəsaɪz]v. 转移
benign[bɪ'naɪn]a. (肿瘤等)良性的
lesion['liːʒən]n. 损害,损伤
osteochondroma[,ɔːstiːəʊkɔːn'drəʊmə]n. 骨软骨瘤
enchondroma[,enkɒn'drəʊmə]n. 内生软骨瘤
radiologic(al)[reɪdiːəʊ'lɔːdʒɪk(əl)]a. 放射学的
orthopedic['ɔːθəʊ'piːdɪk]a. 整形外科的
oncologist[ɒŋ'kɒlədʒɪst]n. 肿瘤学家
biopsy['baɪ,ɒpsɪ]n. 活组织检查v. 对……进行活组织检查
pelvis['pelvɪs]([复]pelvises/pelves)n. 骨盆;盆腔
cortical['kɔːtɪkəl]a. 皮质的,皮层的
osteosarcoma[,ɒstɪəʊsɑː'kəʊmə]n. 骨肉瘤
sarcoma[sɑː'kəʊmə]n. 肉瘤
bimodal[baɪ'məʊdəl]a. 双峰的
metaphyseal[,metə'fɪzɪəl]n. 干骺端的
extremity[ɪk'stremətɪ]([复]extremities)n.肢;(人的)手足
heterogeneous[,hetərəʊ'dʒiːnjəs]a. 多种多样的;混杂的;异原的;异种的;异型的
craniofacial[,kreɪnɪəʊ'feɪʃəl]a. 颅面的
pelvic['pelvɪk]a. 骨盆的
osteoblastic[,ɔːstiːəʊ'blæstɪk]a. 成骨细胞的
osteolytic[,ɔːstiːəʊ'lɪtɪk]a. 溶骨的
periosteal[,perɪ'ɔːstɪəl]a. 骨膜的
plain film 平片
germline['dʒзːmlaɪn]n. 种系
retinoblastoma[,retɪnəʊblæ'stəʊmə]n. 视网膜母细胞瘤
helicase['helɪkeɪs]n. 解[螺]旋酶,蜗牛酶
sporadic[spəʊ'rædɪk,spɔː-]a. 散发的,不定时发生的;(疾病)偶发的
proliferative[prəʊ,lɪfə'reɪtɪv]a. 增生的,增殖的
neoplasm['niːəʊplæzəm]n. 赘生物,(肿)瘤
hematogenously[,hemə'tɒdʒɪnəslɪ,hiːm-]ad.造血地
resection[rɪ'sekʃən]n. 切除术
chemotherapy[,keməʊ'θerəpɪ]n. 化学疗法,化疗
doxorubicin[,dɒksəʊ'ruːbɪsɪn]n. 多柔比星,阿霉素(一种抗肿瘤药)
cisplatin[sɪs'plætɪn]n. 顺铂(一种抗肿瘤药)
neoadjuvant[,niːəʊ'ædʒuːvənt]n. 新辅助疗法
phosphatase['fɒsfəteɪs]n. 磷酸(酯)酶
amputation[,æmpjʊ'teɪʃən]n. 截肢(术)
palliative['pælɪətɪv]a. 治标的;缓解的
chondrosarcoma[,kɔːndrəʊsɑː'kəʊmə]n. 软骨肉瘤
hyaline['haɪəlɪn]a. 透明的
cartilage['kɑːtɪlɪdʒ]n. 软骨
proximal['prɒksɪməl]a. 最接近的;近端的
femur['fiːmə]([复]femurs/femora)n. 股骨
humerus['hjuːmərəs]([复]humeri)n. 肱骨
radiolucency[,reɪdɪəʊ'ljuːsənsɪ]n. 射线透射性
punctate['pʌŋkteɪt]a. 点状的
mineralization[,mɪnərəlaɪ'zeɪʃən]n. 矿化
axial['æksɪəl]a. 轴的,中轴的
peripheral[pə'rɪfərəl]a. (神经)末梢区域的;外围的
mutation[mjuː'teɪʃən]n. 突变,变异
cellularity[,seljʊ'lærətɪ]n. 细胞性
atypia[eɪ'tɪpɪə]n. 异型,非典型
Ewing's sarcoma 尤因肉瘤
neuroectodermal['njuːərəʊ,ektə'dзːməl]a. 神经外胚层的
unimodal[,juːnɪ'məʊdəl]a. (频率曲线或分布)单峰的
diaphyseal[,daɪə'fɪzɪəl]a. 骨干的
rib[rɪb]n. 肋骨
permeative[,pзːmɪ'eɪtɪv]a. 弥漫的;遍布的;渗透的
intermittent[,ɪntə'mɪtənt]a. 间歇的;断断续续的;周期性的
anemia[ə'niːmɪə]n. 贫血症
leukocytosis[,ljuːkəʊsaɪ'təʊsɪs]n. 白细胞增多
sedimentation[,sedɪmen'teɪʃən]n. 沉淀,沉降
polymerase['pɒlɪməreɪs]n. 聚合酶
hybridization[,haɪbrɪdaɪ'zeɪʃən]n. 杂交
regimen['redʒɪmən,-men]n. 生活规则,养生法
receptor[rɪ'septə]n. 感受器;受体
 Exercises
Exercises
Ⅰ.Reading Comprehension
A.Answer the following questions.
1.In the older patients,where's the site of origin for osteosarcoma?
2.What can be used to monitor disease status in osteosarcoma patients?
3.What is the characteristic of chondrosarcoma?
4.What's the difference between osteosarcoma,chondrosarcoma and Ewing's sarcoma?
5.Where does Ewing's sarcoma tend to arise?
B.Choose the right answer to each question.
1.__________ are common on plain films or MRI.
A.Periosteal elevation,cortical destruction and osteolytic lesions
B.Cortical destruction,osteolytic lesions and tumor extension into soft tissue
C.Osteolytic lesions,tumor extension into soft tissue and periosteal elevation
D.Tumor extension into soft tissue,periosteal elevation and cortical
destruction
2.The development of effective systemic chemotherapy with and ,with or without methotrexate,has had a profoundly positive effect on treatment outcome,with 5-year disease-free survival rates exceeding 65%in patients younger than40 years with non-metastatic extremity tumors.
A.vincristine;doxorubicin
B.doxorubicin;cyclophosphamide
C.doxorubicin;cisplatin
D.cyclophosphamide;vincristine
3.The most common primary sites of chondrosarcoma are in , , and .
A.the pelvis;the lung;proximal femur
B.the lung;proximal femur;proximal humerus
C.the pelvis;proximal femur;proximal humerus
D.the pelvis;proximal humerus;the lung
4.Radiographically,chondrosarcoma is detected as an area of radiolucency with variable punctate mineralization,with or , sometimes with extension into adjacent soft tissue.
A.frequent cortical bone erosion;celluar atypia
B.celluar atypia;frequent cortical bone thickening
C.frequent cortical bone erosion;frequent cortical bone thickening
D.osteoblastic lesions;celluar atypia
5.Ewing's tumors are characterized radiologically by a or“ ”appearance of the affected bone,with a multilayered“onion-skin”periosteal reaction.
A.permeative;moth-eaten
B.moth-eaten;punctate
C.punctate;heterogeneous
D.heterogeneous;permeative
Ⅱ.Words and Expressions
A.Fill in the blanks with the words or expressions given below,and change the form where necessary.
osteosarcoma sarcoma craniofacial pelvic periostea
metastasis resection chemotherapy benign enchondroma
skeleton diaphyseal anemia leukocytosis antagonist
1.The structure of the__________ bones showed the skeleton was that of a female.
2.Approximately one third of all patients with malignant disease have hepatic__________ .
3.Although radiation therapy and__________ probably produce definitive effects,the death rate of cancer patients is still extremely high.
4.Lipoma is the second most common__________ tumor of the colon.
5.Proliferation of fibroblastic cells in bone marrow,causing__________ and sometimes enlargement of the spleen and liver.
6.__________ is a type of benign bone tumor that originates from cartilage.
7.In addition,__________ may interact at unique binding sites not normally involved in the biological regulation of the receptor's activity to exert the effects.
8.__________ and other connective tissue neoplasms are an overwhelmingly complex and heterogeneous mixture of diseases with a wide range of clinical behaviors and outcomes.
9.Striated skeletal muscle is commonly called“skeletal”because most of it is attached by at least one end to some part of the__________ .
10.Pain,anorexia,fever,__________ ,and abdominal tenderness are usually present in appendicitis during pregnancy.
B.Fill in the blanks with the suitable words or expressions from each group.
A person who has or has had cancer and develops bone pain or 1 is evaluated for 2 bone tumors.Bone scans using 3 tracers and X-rays can help locate these tumors.Magnetic resonance imaging(MRI)or positron emission tomography(PET)is even more accurate.Occasionally,a metastatic bone 4 causes symptoms before the original cancer has been detected. 5 may consist of pain or a 6 where the tumor has weakened the bone(a pathologic fracture).In these situations,a 7 usually gives clues as to the location of the original cancer,because the type of cancer 8 can often be recognized under the microscope and direct the doctor to the 9 cancer(for example,lung,breast,prostate,kidney,thyroid,or colon).
Treatment depends on the type of cancer that has spread to the bone.Some types respond to chemotherapy,some to 10 therapy,some to both,and some to neither.Radiation therapy is usually most effective. 11 to stabilize the bone can sometimes prevent fractures.Some metastatic bone lesions require removal of part of a 12 and rebuilding of the limb and joint.When the original(primary)cancer has been removed and only a single metastasis in the bone exists(especially when the metastasis develops years after the original tumor),surgical removal with reconstruction,sometimes combined with radiation therapy,chemotherapy,or both,rarely may be 13 but may significantly improve the quality of life as well as the function or appearance of the limb.
One of the goals of treatment is to minimize loss of bone tissue.Loss of bone tissue can cause pain and make 14 prone to fractures,which can require surgery.Bone loss can be minimized by using radiation 15 and drugs that prevent bone loss(such as bisphosphonates)before bone loss is extensive and pain occurs.If tumors cause the vertebra to collapse but not to put pressure against the spinal 16 ,kyphoplasty(a surgery designed to stop the pain cause by a spinal fracture)can be used.In vertebroplasty(injection alone)or kyphoplasty(use of an expanding balloon first),bone cement(methyl methacrylate)is 17 into the bone to make the area expand,which can relieve 18 and prevent further collapse.If the tumors appear to be at risk of collapse that could cause spinal cord damage(such as paraplegia),treatment to decompress the 19 and stabilize the 20 may be recommended.
1.A.swelling B.calcifying C.bleeding D.contracting
2.A.initial B.original C.metastatic D.benign
3.A.progressive B.radioactive C.preoperative D.postoperative
4.A.necrosis B.lesion C.node D.tumor
5.A.Syndromes B.Complications C.Symptoms D.Illnesses
6.A.fracture B.spasm C.hemorrhage D.edema
7.A.CT B.biopsy
C.urinalysis D.electrocardiogram
8.A.joint B.nerve C.tissue D.dermis
9.A.metastatic B.secondary C.malignant D.primary
10.A.radiation B.medicine C.injection D.chemotherapy
11.A.Checkup B.Surgery C.Diagnosis D.Prognosis
12.A.thigh B.trunk C.limb D.muscle
13.A.beneficial B.relieved C.curative D.effective
14.A.bones B.neurons C.extremities D.cartilages
15.A.treatment B.operation C.therapy D.examination
16.A.cord B.motor C.column D.posture
17.A.placed B.inserted C.injected D.invaded
18.A.hurt B.pain C.stress D.trauma
19.A.pain B.bruise C.pressure D.hypertension
20.A.spine B.rib C.skeleton D.tissue
Ⅲ.Translation
A.Translate the following sentences into Chinese.
1.The development of effective systemic chemotherapy with doxorubicin and cisplatin,with or without methotrexate,has had a profoundly positive effect on treatment outcome,with 5-year disease-free survival rates exceeding 65%in patients younger than 40 years with non-metastatic extremity tumors.
2.Chondrosarcoma,a malignant tumor characterized by hyaline cartilage differentiation,is the second most common sarcoma of bone,representing 25%of bone sarcomas.The peak incidence is in the fifth to seventh decades of life.The most common primary sites are in the pelvis,proximal femur,and proximal humerus.
3.After completion of staging procedures,patients are treated with neoadjuvant chemotherapy.After 3 months of chemotherapy,the primary tumor is resected,radiated,or both,depending on the location and extent of the primary tumor.Chemotherapy is then resumed for a total of up to1 year of treatment.
B.Translate the following sentences into English.
1.骨肿瘤是发生于骨骼或其附属组织的肿瘤。同发生于身体其他组织的肿瘤一样,其确切病因不明。骨肿瘤可分为良性与恶性两类。良性肿瘤易治愈,且预后良好;恶性肿瘤发展迅速,死亡率高。
2.手术切除是治疗恶性肿瘤的主要手段。化学治疗(化疗)分为全身化疗和局部化疗。常用的药物有多柔比星(阿霉素)和大剂量甲氨蝶呤。放射疗法只能作为一种辅助治疗手段。
Ⅳ.Writing
A.Write an abstract of Text A.
B.Write a topic-related and literature-based report on Prognosis of Malignant Bone Sarcoma,Especially Osteosarcoma and Ewing's Sarcoma.