Text A Surgical Treatmentof Coronary Artery Disease
Coronary Artery Bypass Grafting
Coronary artery bypass grafting(CABG)is based on the premise that the morbidity and mortality associated with coronary atherosclerosis are largely related to atherosclerotic coronary stenoses that can be demonstrated by coronary angiography and that if grafts are constructed to route blood flow around these stenoses,myocardial blood supply can be improved or preserved, cardiac symptoms relieved,cardiac events diminished,and survival prolonged. Over time,the fundamentals of that concept have been shown to be correct.
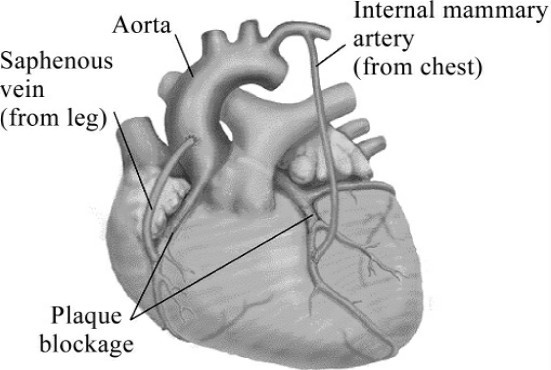
Fig.2-1 Coronary artery bypass grafting
The most common types of grafts for coronary artery bypass have been reversed segments of saphenous vein and the internal thoracic arteries. Saphenous vein grafts are anastomosed to the aorta(proximal anastomosis) and to the coronary artery distal to the major obstruction(Fig.2-1). Saphenous vein grafts have the advantages of availability,larger size than most coronary arteries,and favorable handling characteristics.However,with time,saphenous vein grafts may develop intrinsic pathologic changes,intimal fibroplasia,and vein graft atherosclerosis, each of which may lead to narrowing or occlusions.By 10 years after surgery, approximately 30%of saphenous vein grafts become occluded,and 30%to 35% of those remaining exhibit angiographic evidence of vein graft atherosclerosis.Treatment with platelet inhibitors and statins decreases the risk of vein graft failure but does not eliminate it.
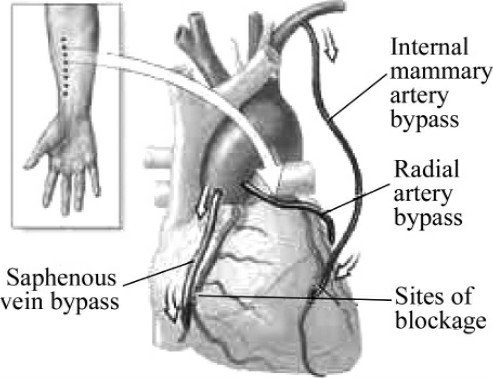
Fig.2-2 Different types of artery bypass
Internal thoracic artery grafts,on the other hand,are resistant to the development of late atherosclerosis. When it is used as an in situ(subclavian origin intact)graft to the left anterior descending(LAD)coronary artery,the left internal thoracic artery graft has a more than 90%patency rate up to 20 years after operation(Fig.2-2).Because the LAD coronary artery has a strong prognostic influence,the left internal thoracic artery to LAD graft is a clinically important part of myocardial revascularization.Patients who receive a left internal thoracic artery to LAD graft with or without saphenous vein grafts have a better long-term survival rate,fewer reoperations,and fewer cardiac events compared with patients receiving only saphenous vein grafts.The right internal thoracic artery may also be used for revascularization as an in situ graft,as an aorta to coronary artery graft,or as a composite arterial graft from the left internal thoracic artery to a coronary artery.Use of both internal thoracic arteries as grafts provides incremental benefit over a single internal thoracic artery graft strategy and produces an improved survival with a lower risk for reoperation.By comparison,radial artery grafts provide outcomes that are essentially equivalent to those with saphenous vein grafts(Fig.2-3).
Most CABG operations have been performed with a full median sternotomy incision,historically with the aid of cardiopulmonary bypass, aortic cross-clamping,and cardioplegic solution—techniques that allow exposure and arrest of the heart such that detailed microsurgical anastomoses can be constructed while myocardial function is effectively protected.By comparison, strategies for performing operations through smaller incisions(minimally invasive surgery)have had limited application for coronary revascularizations. Although beating heart (off-pump) surgery without cardiopulmonary bypass has been widely advocated to avoid neurologic complications,it apparently does not provide such protection and leads to lower rates of graft patency compared with traditional on-pump CABG.
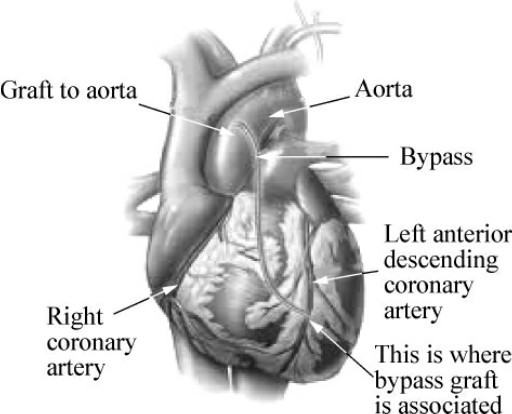
Fig.2-3 LAD bypass graft
Indications for Bypass Surgery
The goals of CABG are to relieve symptoms and to prolong life expectancy.On the basis of randomized trials and the emergence of alternative medical treatments and percutaneous coronary intervention(PCI),the surgical population has evolved toward patients with complex conditions,often involving left main or triple-vessel disease,diffuse coronary stenoses,totally obstructed vessels,abnormal left ventricular function,and diabetes.Surgically treated patients with single-vessel disease usually have LAD stenoses or have failed alternative treatments.
Perioperative Risks
The risk of mortality associated with CABG correlates with ischemia at the time of operation,left ventricular function,extent of coronary stenoses,non-cardiac atherosclerosis,and comorbid conditions and with the experience,skill, and judgment of the surgeon.Effective myocardial protection has diminished much of the incremental risk based on the severity of cardiac disease.For patients younger than 70 years without serious comorbid conditions,the mortality risk of primary CABG surgery is less than1%in experienced hands regardless of the number of coronary arteries that are stenotic,and left ventricular dysfunction only slightly increases risk.Nevertheless,CABG surgery in the presence of ongoing myocardial ischemia due to acute myocardial infarction,unstable angina,or acute vessel closure after PCI is still associated with increased risk.National data on primary CABG operations show a 1.7% mortality rate for elective operations,a2.6%rate for“urgent”operations,a6%rate for“emergency”procedures,and a 23%rate for“salvage”operations.Noncardiac comorbid conditions (aortic atherosclerosis,renal function,chronic obstructive pulmonary disease,and coagulation system disorders)increase perioperative risk when these conditions are severe.
The most serious postoperative morbidity after CABG is stroke,often related to aortic or cerebrovascular atherosclerosis and atherosclerotic embolization. Heightened awareness of the importance of aortic and carotid atherosclerosis and improved management strategies appear to have decreased the risk of focal stroke in patients previously at high risk.Serious wound complications of median sternotomy are uncommon(1%to 2%).Obesity,diabetes,and bilateral internal thoracic artery grafting(particularly in combination with diabetes)are associated with higher rates of wound complications.
Late Outcomes
The late outcomes after CABG are related to age,severity of cardiac disease before operation,noncardiac comorbid conditions,progression of atherosclerosis,and the operation itself.Many of these factors can be influenced by treatment choices.CABG tends to diminish but not to eliminate long-term survival differences based on the number of diseased coronary vessels,left main stenosis,and different levels of left ventricular function.The achievement of complete revascularization(bypass grafts to all stenotic coronary vessels)and the use of internal thoracic artery grafts improve long-term survival rates and symptomatic status.
Pronged survival.Patients often have pronged survival after CABG;more than 80%of patients are alive more than 10 years after operation.Over the long term,control of the progression of atherosclerosis by lifestyle modifications,pharmacologic treatment of hypertension and lipids and platelet inhibitors appears to extend the benefits of CABG.
Symptom relief.If patients who experience angina have severe stenoses in graftable coronary arteries that supply areas of myocardium ischemic at rest or with stress,CABG will reliably relieve angina.Randomized trials have shown that the relief of angina after CABG is more consistent than that achieved with alternative treatments.When intermittent heart failure symptoms represent an“anginal equivalent”that is also caused by ischemia,such symptoms also respond well to relief of that ischemia by CABG.Patients with symptoms of heart failure at rest are more complex,but dobutamine echocardiography and positron emission tomography can identify segments of viable but hibernating myocardium(ischemic at rest)that may improve with bypass grafting,thus reducing symptoms of heart failure.
(1,130 words)
New Words and Phrases
coronary['kɒrənərɪ]a. 冠状的;心脏冠状动脉的
artery['ɑːtərɪ]n. 动脉
coronary artery disease(CAD) 冠心病
graft[ɡrɑːft]n.&v. 移植;嫁接
coronary artery bypass grafting(CABG) 冠状动脉旁路移植术
atherosclerosis[,æθərəʊsklə'rəʊsɪs] 动脉粥样硬化
([复]atheroscleroses)n.
atherosclerotic[,æθərəʊsklə'rɒtɪk]n. 动脉粥样硬化患者a . 动脉粥样硬化的
stenosis[stɪ'nəʊsɪs]([复]stenoses)n. (器官)狭窄
angiography[,ændʒɪ'ɒɡrəfɪ]n. 血管造影术
myocardial[,maɪəʊ'kɑːdɪəl]a. 心肌的
saphenous[sə'fiːnəs]a. 隐静脉的
vein[veɪn]n. 静脉
thoracic[θɔː'ræsɪk]a. 胸的,胸廓的
anastomose[ə'næstəməʊz]v. (使血管等)吻合
aorta[eɪ'ɔːtə]n. 主动脉
anastomosis[,ænəstə'məʊsɪs]n. 接合,相接;吻合
pathologic[,pæθə'lɒdʒɪk]a. 病理的
intimal['ɪntɪməl]a. 内膜的
fibroplasia[,faɪbrəʊ'pleɪʒə]n. 纤维组织增生,纤维增生
occusion[ə'kluːʒən]n. 闭塞;闭合
occlude[ə'kluːd]v. 闭塞;闭合;咬合
angiographic[,ændʒɪəʊ'ɡrɑːfɪk]a. 血管造影术的
platelet['pleɪtlət]n. 血小板;小盘,小板
statin[stætɪn]n. 抑制素(14肽生长抑素)
in situ[ɪn'saɪtjuː]a. 在原位置,原位的
subclavian[,sʌb'kleɪvɪən]a. 锁骨下的
revascularization[riː,væskjʊləraɪ'zeɪʃən]n. 血管的再形成,血管再生
radial['reɪdɪəl]a. 桡骨的
sternotomy[stзː'nɒtəmɪ]n. 胸骨切开术
incision[ɪn'sɪʒən]n. 切开;切口
cardiopulmonary[,kɑːdɪəʊ'pʌlmənərɪ]a. 心肺的
cardiopulmonary bypass 心肺转流术;体外循环
aortic cross-clamping 主动脉横断钳闭术;主动脉交叉钳夹
cardioplegic['kɑːdiːəʊ'pledʒɪk]a. 心脏停搏的
cardioplegic solution 心脏停搏液
arrest[ə'rest]v.&n. 停止,阻止
off-pump 非体外循环,心肺转流
neurologic[,njʊərə'lɒdʒɪk]a. 神经病学的;神经系统的
on-pump 体外循环
percutaneous[,pзːkjuː'teɪnɪəs]a. 经皮的,经由皮肤的
percutaneous coronary intervention(PCI) 经皮冠状动脉介入术
ventricular[ven'trɪkjʊlə]a. 心室的;脑室的
perioperative[,perɪ'ɒpərətɪv]a. 手术期间的,围手术期的
ischemia[ɪs'kiːmɪə]n. 缺血
incremental[,ɪŋkrɪ'mentəl]a. 增加的;递增的
stenotic[stə'nɒtɪk]a. 狭窄的
dysfunction[dɪs'fʌŋkʃən]n. 功能障碍,功能失调
infarction[ɪn'fɑːkʃən]n. 梗死形成
acute myocardial infarction 急性心肌梗死
angina[æn'dʒaɪnə]n. 心绞痛;咽痛,咽峡炎
pulmonary['pʌlmənərɪ]a. 肺的
coagulation[kəʊ,æɡjʊ'leɪʃən]n. 凝结,凝固
stroke[strəʊk]n. 脑卒中(中风)
aortic[eɪ'ɔːtɪk]a. 主动脉的
cerebrovascular[,serɪbrəʊ'væskjuːlə]a. 脑血管的
embolization[,embəlaɪ'zeɪʃən]n. 栓塞(现象)
carotid[kə'rɒtɪd]n.&a. 颈动脉(的)
focal['fəʊkəl]a. 病灶的,病灶性的
pharmacologic[,fɑːməkə'lɒdʒɪk]a. 药理学的,药物学的
lipid['lɪpɪd]n. 脂质;油脂
myocardium[,maɪəʊ'kɑːdɪəm]n. 心肌(层)
dobutamine[dəʊ'bjuːtəmiːn]n. 多巴酚丁胺
echocardiography['ekəʊ,kɑːdɪ'ɒɡrəfɪ]n. 心回波描记术,超声心动描记术
tomography[təʊ'mɒɡrəfɪ]n. X线断层照相术
positron emission tomography 正电子成像术,正电子放射断层造影
 Exercises
Exercises
Ⅰ.Reading Comprehension
A.Answer the following questions.
1.What premise is coronary artery bypass grafting(CABG)based on?
2.What are the most common types of grafts for coronary artery bypass?
3.How are most CABG operations performed?
4.How many factors influence the risk of mortality associated with CABG?
5.What are related to the late outcomes after CABG?
B.Decide whether the following statements are True or False.
1.Treatment with platelet inhibitors and statins eliminates the risk of vein graft failure.
2.Patients who receive a left internal thoracic artery to LAD graft have a better long-term survival rate.
3.Radial artery grafts provide outcomes that are essentially equivalent to those with saphenous vein grafts.
4.The most serious postoperative morbidity after CABG is cerebrovascular atherosclerosis.
5.Complete revascularization(bypass grafts to all stenotic coronary vessels) and the use of internal thoracic artery grafts decrease long-term survival rates and symptomatic status.
Ⅱ.Words and Expressions
A.Fill in the blanks with the words or expressions given below,and change the form where necessary.
stroke symptomatic atherosclerosis stenosis cardiopulmonary
cerebrovascular angiography thoracic incision infarction
coronary embolization angina revascularization graft
1.The doctor__________ apiece of skin from his thigh onto his wound.
2.Using a micro-robot,by contrast,might involve only one__________ and smaller surgical instruments.
3.If someone has a__________ ,a blood vessel in their brain bursts or becomes blocked, this may kill them or make them unable to move one side of their body.
4.Lung injury during__________ bypass may result in severe complication after open heart surgery.
5.In older people,the causes are the same as for other__________ problems:hypertension,high cholesterol and smoking.
6.Behavioral risk factors are responsible for about 80%of coronary heart disease and__________ disease.
7.The artery should get wider when blood flow in the area increases,but diseases such as__________ hamper this effect.
8.__________ is severe pain in the chest and left arm,caused by heart disease.
9.Carotid atherosclerosis is a common cause of cerebral__________ .
10.During coronary__________ ,a thin tube(catheter)is threaded through a blood vessel into the heart,where a special dye is injected.
B.Fill in the blanks with the suitable words or expressions from each group.
Coronary artery disease is a chronic process that begins during adolescence and slowly progresses throughout life.Independent 1 factors include a family history of 2 coronary artery disease,cigarette smoking,diabetes 3 , hypertension,hyperlipidemia(高脂血,血脂过多),sedentary lifestyle,and 4 . These risk factors accelerate or modify a complex and chronic inflammatory process that ultimately manifests as fibrous atherosclerotic 5 .
The most widely accepted theory of atherosclerosis states that the process represents an attempt at healing in response to 6 injury.The first step in the atherosclerotic process is the development of fatty 7 ,which contain atherogenic(导致动脉粥样化的) 8 and macrophage foam cells.These streaks form between the endothelium and internal elastic lamina.Over time, an intermediate 9 made up of an extracellular lipid core and layers of smooth 10 and connective tissue matrix eventually 11 a fibrous cap. The edge of the fibrous cap(the shoulder region)plays a critical role in the development of 12 coronary syndromes.The shoulder region is the site where most plaques lose their integrity,or rupture.Plaque 13 exposes the underlying thrombogenic core of lipid and 14 material to circulating blood. This exposure results in platelet adherence,aggregation,and progressive luminal narrowing,which are associated with acute coronary 15 .
16 is emerging as a critical component of atherosclerosis genesis, activity,and potential plaque instability.Patients with 17 coronary artery disease who possess a confluence of risk factors known as the 18 syndrome remain at particularly high risk for a future 19 event,such as an acute myocardial infarction or cerebrovascular accident.Biochemical markers such as elevated levels of C-reactive protein signal a higher 20 of vascular inflammation and portend a higher risk of vascular event rates.This marker may also signal more rapidly advancing coronary artery disease and the need for aggressive preventive measures.
1.A.risk B.danger C.hazard D.threat
2.A.previous B.original C.premature D.untimely
3.A.glycuresis B.illness C.disease D.mellitus
4.A.fatness B.obesity C.heaviness D.plumpness
5.A.sign B.platelet C.plaque D.tablet
6.A.endothelial B.dermal C.tegumentary D.cortical
7.A.signs B.lines C.wrinkles D.streaks
8.A.cells B.lipoproteins C.fat D.proteins
9.A.cut B.scratch C.lesion D.injury
10.A.muscle B.tissue C.fibrous cap D.skin
11.A.appears B.forms C.shapes D.moulds
12.A.severe B.chronic C.sharp D.acute
13.A.rupture B.break C.split D.crack
14.A.dying B.malignant C.necrotic D.rotten
15.A.symptoms B.disorders C.complications D.syndromes
16.A.Irrigation B.Inflammation C.Tenderness D.Soreness
17.A.recognized B.well-known C.established D.reputable
18.A.myocardial B.metabolic C.potential D.critical
19.A.mental B.neural C.physical D.vascular
20.A.likelihood B.chance C.odds D.possibility
Ⅲ.Translation
A.Translate the following sentences into Chinese.
1.Saphenous vein grafts have the advantages of availability,larger size than most coronary arteries,and favorable handling characteristics.However, with time,saphenous vein grafts may develop intrinsic pathologic changes, intimal fibroplasia,and vein graft atherosclerosis,each of which may lead to narrowing or occlusions.
2.Use of both internal thoracic arteries as grafts provides incremental benefit over a single internal thoracic artery graft strategy and produces an improved survival with a lower risk for reoperation.By comparison,radial artery grafts provide outcomes that are essentially equivalent to those with saphenous vein grafts.
3.Most CABG operations have been performed with a full median sternotomy incision,historically with the aid of cardiopulmonary bypass,aortic cross-clamping,and cardioplegic solution—techniques that allow exposure and arrest of the heart such that detailed microsurgical anastomoses can be constructed while myocardial function is effectively protected.
B.Translate the following sentences into English.
1.对患有严重静脉移植物动脉粥样硬化患者的观察研究表明,这是一种不稳定的病变损伤,往往导致严重心脏疾病发作,特别是当有左前降支或多条血管受损时。
2.对于慢性冠状动脉综合征的患者,目前还没有资料证实经皮冠状动脉介入治疗可延长生命。但随机试验表明,冠状动脉旁路移植术(CABG)可延长严重冠状动脉疾病患者的寿命。
Ⅳ.Writing
A.Write an abstract of Text A.
B.Write a topic-related and literature-based report on Coronary Artery Disease.