Text A Acute Renal Failure
The Characteristics of Acute Renal Failure(ARF)and the Classification of Its Causes
Acute renal failure(ARF)is characterized by a rapid decline in glomerular filtration rate(GFR)over hours to days.Depending on the exact definition used,ARF complicates approximately 5%—7%of hospital admissions and up to 30%of admissions to intensive care units.Retention of nitrogenous waste products,oliguria(urine output<400 m L/d contributing to extracellular fluid overload),and electrolyte and acid-base abnormalities are frequent clinical features.ARF is usually asymptomatic and diagnosed when biochemical monitoring of hospitalized patients reveals a new increase in blood urea and serum creatinine concentrations.For purposes of diagnosis and management, causes of ARF are generally divided into three major categories:(1)diseases that cause renal hypoperfusion,resulting in decreased function without frank parenchymal damage(prerenal ARF,or azotemia)(~55%);(2)diseases that directly involve the renal parenchyma(intrinsic ARF)(~40%);and (3)diseases associated with urinary tract obstruction(postrenal ARF)(~5%) (Fig.1-1,1-2).ARF is often considered to be reversible,although a return to baseline serum creatinine concentrations postinjury might not be sufficiently sensitive to detect clinically significant irreversible damage that may ultimately contribute to chronic kidney disease.ARF is associated with significant in-hospital morbidity and mortality,the latter in the range of 30%—60%, depending on the clinical setting and presence or absence of nonrenal organ system failure.
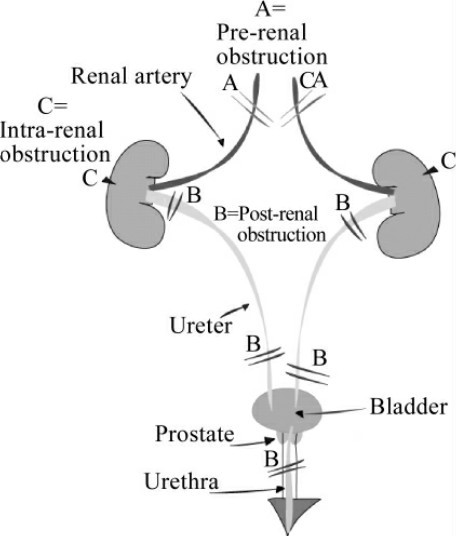
Fig.1-1 The categories of ARF
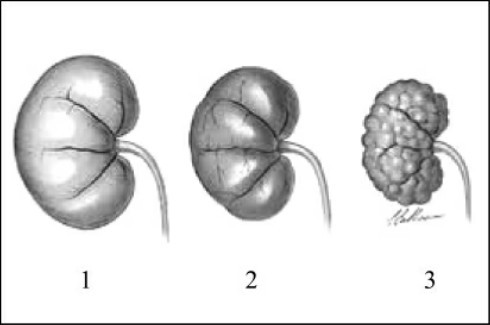
Fig.1-2 The process of ARF
Etiology and Pathophysiology
The most common form of ARF(prerenal azotemia)is prerenal ARF, which occurs in the setting of renal hypoperfusion.Prerenal ARF is generally reversible when renal perfusion pressure is restored.By definition,renal parenchymal tissue is not damaged.More severe or prolonged hypoperfusion may lead to ischemic injury,often termed acute tubular necrosis,or ATN. Thus,prerenal ARF and ischemic ATN fall along a spectrum of manifestations of renal hypoperfusion.Prerenal ARF can complicate any disease that induces hypovolemia,low cardiac output,systemic vasodilatation,or selective intrarenal vasoconstriction.
Clinical Assessment
Symptoms of prerenal ARF include thirst and orthostatic dizziness. Physical signs of orthostatic hypotension,tachycardia,reduced jugular venous pressure,decreased skin turgor and dry mucous membranes suggest prerenal ARF.Careful clinical examination may reveal stigmata of chronic liver disease and portal hypertension,advanced cardiac failure,sepsis,or other causes of reduced“effective”arterial blood volume.Case records should be reviewed for documentation of a progressive fall in urine output and body weight and recent initiation of treatment with diuretics,NSAIDs,ACE inhibitors,or ARBs.
Prevention
Because there are no specific therapies for ischemic or nephrotoxic ARF, prevention is of paramount importance.Many cases of ischemic ARF can be avoided by close attention to cardiovascular function and intravascular volume in high-risk patients,such as the elderly and those with preexisting chronic kidney disease.Indeed,aggressive restoration of intravascular volume has been shown to dramatically reduce the incidence of ischemic ARF after major surgery or trauma,burns,or cholera.The incidence of nephrotoxic ARF can be reduced by tailoring the administration(dose and frequency)of nephrotoxic drugs to body size and GFR.In this regard,it should be noted that serum creatinine is a relatively insensitive index of GFR and may overestimate GFR considerably in small or elderly patients.For purposes of drug dosing,it is advisable to estimate the GFR using the Cockcroft-Gault formula(which factors in age,sex,and weight)or the simplified Modification of Diet in Renal Disease(MDRD)equation(which factors in age,sex,weight,and race).Of note,these equations cannot be used to estimate GFR when creatinine is not at steady state(e.g.during evolving ARF).
Adjusting drug dosage according to circulating drug levels also appears to limit renal injury in patients receiving aminoglycoside antibiotics,cyclosporine,or tacrolimus.Diuretics,NSAIDs,ACE inhibitors,ARBs,and vasodilators should be used with caution in patients with suspected true or“effective”hypovolemia or renovascular disease as they may precipitate prerenal ARF or convert the latter to ischemic ARF.Allopurinol and forced alkaline diuresis are useful prophylactic measures in patients at high risk for acute urate nephropathy(e.g.cancer chemotherapy in hematologic malignancies)to limit uric acid generation and prevent precipitation of urate crystals in renal tubules. Rasburicase,a recombinant urate-oxidase enzyme,catalyzes enzymatic oxidation of uric acid into a soluble metabolite(allantoin).Forced alkaline diuresis may also prevent or attenuate ARF in patients receiving high-dose methotrexate or suffering from rhabdomyolysis.N-acetylcysteine limits acetaminophen-induced renal injury if given within 24 h of ingestion.
A number of preventive measures have been proposed for contrast nephropathy.It is clear that hydration is an effective preventive measure. Other measures that have been proposed include loop diuretics and mannitol, dopamine,fenoldopam,N-acetylcysteine,theophylline,and sodium bicarbonate. Despite favorable experimental data,there is insufficient evidence to support the use of loop diuretics or mannitol to prevent radiocontrast nephropathy or any other cause of ARF.Likewise,despite its widespread use,dopamine has proved ineffective as a prophylactic agent.Fenoldopam,a dopamineα1specific agonist approved for use as a parenteral antihypertensive agent,has been tested in several clinical trials and does not appear to reduce the incidence of contrast nephropathy.Moreover,fenoldopam is associated with significant side effects, including systemic hypotension,and its use as an agent to prevent radiocontrast nephropathy should be discouraged.In contrast,several(relatively small) randomized clinical trials(RCTs)have suggested a clinical benefit to the use of N-acetylcysteine,although have been inconclusive.
However,aside from the potential hazards associated with a delay in radiographic imaging,N-acetylcysteine appears to be safe,and its use in patients at high risk for radiocontrast nephropathy is reasonable,based on its low side effect profile.Larger RCTs will be required to show definitive benefit. Theophylline and aminophylline(adenosine antagonists)offer the potential advantage of use immediately preceding radiocontrast administration,although the benefit,if present,appears marginal in most studies.Lastly,volume expansion with bicarbonate-containing intravenous fluids has been suggested to be superior to sodium chloride(saline)administration and showed a significant benefit in a single center RCT.Unlike N-acetylcysteine,the use of sodium bicarbonate does not obligate a delay in imaging(the published protocol began intravenous fluids 1 h before the imaging study was begun).Whether a combination of strategies(e.g.N-acetylcysteine+sodium bicarbonate)offers additive benefit and that patients require treatment remain unclear and warrant further study.
Specific Therapies
By definition,prerenal ARF is rapidly reversible upon correction of the primary hemodynamic abnormality,and postrenal ARF resolves upon relief of obstruction.To date there are no specific therapies for established acute kidney injury(AKI).Management of these disorders should focus on elimination of the causative hemodynamic abnormality or toxin,avoidance of additional insults,and prevention and treatment of complications.Specific treatment of other causes of intrinsic renal ARF depends on the underlying pathology.
(1,177 words)
New Words and Phrases
renal['riːnəl]a. 肾脏的
glomerular[ɡlɒ'merjʊlə]a. 肾小球的
nitrogenous[naɪ'trɒdʒənəs]a. 含氮的,氮的
oliguria[,ɒlɪ'ɡjʊərɪə]n. 尿过少,少尿(症)
extracellular[,ekstrə'seljʊlə]a. (位于或发生于)细胞外的
electrolyte[ɪ'lektrəʊlaɪt]n. 电解质;电解(溶)液
acid-base['æsɪd-beɪs]a. 酸碱的
asymptomatic[,eɪsɪmptə'mætɪk]a. 无临床症状的
serum['sɪərəm]([复]-rums/-ra)n. 血清;浆液
creatinine[kriː'ætɪniːn]n. 肌酸酐,肌酐
hypoperfusion[,haɪpəʊpə'fjuːʒən]n. 灌注不足
parenchymal[pə'reŋkɪməl]a. 实质的;主质的
azotemia[,æzə'tiːmɪə]n. 氮质血症
parenchyma[pə'reŋkɪmə]n. 实质;主质;薄壁组织
morbidity[mɒ'bɪdɪtiː]n. 病态,发病;发病率
mortality[mɔː'tælɪtiː]n. 死亡率,病死率
etiology[,iːtɪ'ɒlədʒɪ]n. 病因学
pathophysiology['pæθəʊ,fɪzɪ'ɒlədʒɪ]n. 病理生理学
ischemic[ɪ'skiːmɪk]a. 缺血的
tubular['tjuːbjʊlə]a. 小管的,管状的
necrosis[ne'krəʊsɪs]n. 坏死
hypovolemia[,haɪpəʊvə'liːmɪə]n. (循环)血容量减少
cardiac['kɑːdɪæk]a. 心脏(病)的
vasodilatation[,væzəʊdaɪlə'teɪʃən]n. 血管舒张
vasoconstriction[,væzəʊkən'strɪkʃən]n. 血管收缩
orthostatic[,ɔːθəʊ'stætɪk]a. 直立的
hypotension[,haɪpəʊ'tenʃən]n. 血压过低
tachycardia[,tækɪ'kɑːdɪə]n. 心动过速
jugular['dʒʌɡjʊlə]a. 颈的,颈静脉的
venous['viːnəs]a. 静脉的
turgor['tзːɡə]n. 细胞(组织)的膨胀,肿胀
mucous['mjuːkəs]a. 黏液的,分泌黏液的
membrane['membreɪn]n. 膜
stigma['stɪgmə]([复]stigmas/stigmata)n. 皮肤上的红斑;特征
sepsis['sepsɪs]n. 败血症,脓毒症
arterial[ɑː'tɪərɪəl]a. 动脉的
diuretic[,daɪjʊə'retɪk]n. 利尿剂
NSAIDs(non-steroidal anti-inflammatory drugs) 非类固醇消炎药,非甾类消炎药
ACE(angiotensin converting enzyme) 血管紧张素转化酶
inhibitor[ɪn'hɪbɪtə]n. 抑制剂
ARBs(angiotensin receptor blockers) 血管紧张素受体阻断剂
nephrotoxic[,nefrə'tɒksɪk]a. 对肾脏有害的
cardiovascular[,kɑːdɪəʊ'væskjʊlə]a. 心血管的
intravascular[,ɪntrə'væskjʊlə]a. 血管内的
incidence['ɪnsɪdəns]n. 发生率,发病率
cholera['kɒlərə]n. 霍乱
aminoglycoside[ə,miːnəʊ'ɡlaɪkə,saɪd]n. 氨基糖苷类
cyclosporine[saɪkləʊ'spɔːrɪn]n. 环孢素
vasodilator[,veɪzəʊdaɪ'leɪtə]n. 血管扩张剂
renovascular[,riːnəʊ'væskjʊlə]a. 肾血管(性)的
allopurinol[,æləʊ'pjʊərɪnɒl]n. 别嘌醇(治痛风药)
alkaline['ælkəlaɪn]a. 碱性的
diuresis[,daɪjʊə'riːsɪs]n. 多尿;利尿
prophylactic[,prɒfɪ'læktɪk]a. 预防(性)的
urate['jʊəreɪt]n. 尿酸盐
nephropathy[nɪ'frɒpəθɪ]n. 肾病
hematologic[,hemətə'lɒdʒɪk]a. 血液学的
malignancy[mə'lɪɡnənsɪ]n. 恶性
tubule['tjuːbjuːl]n. 小管,细管
rasburicase n. 拉布立酶(一种酶类药)
urate oxidase enzyme['jʊəreɪt'ɒksɪdeɪz en'zaɪm]尿酸氧化酶
enzymatic[,enzaɪ'mætɪk]a. 酶性的
metabolite[mɪ'tæbəlaɪt]n. 代谢物
allantoin[ə'læntəʊɪn]n. 尿囊素
methotrexate[,meθə'trekseɪt]n. 甲氨蝶呤(一种抗肿瘤药)
rhabdomyolysis[,ræbdəʊmaɪ'ɒlɪsɪs]n. 横纹肌溶解
N-acetylcysteine N-乙酰半胱氨酸;胱氨酸
acetaminophen[ə,siːtə'mɪnəfən]n. 对乙酰氨基酚
loop diuretic[luːp daɪjʊə'retɪk]n. 亨氏环利尿剂,髓袢利尿剂
mannitol['mænɪtɒl]n. 甘露醇
dopamine['dəʊpə,miːn]n. 多巴胺
fenoldopam 非诺多泮(一种血管扩张药)
theophylline[,θɪə'fɪliːn]n. 茶碱
sodium bicarbonate['səʊdiːəm baɪ'kɑːbənɪt] 碳酸氢钠,小苏打
radiocontrast nephropathy 造影剂肾病
agonist['æɡənɪst]n. 主动肌;兴奋剂,激动剂
parenteral[pæ'rentərəl]a. 肠胃外的,非肠道的
antihypertensive['æntɪ,haɪpə'tensɪv]a.&n. 抗高血压的(药物)
radiographic[,reɪdɪəʊ'ɡrɑːfɪk]a. X线照相的,放射显影
aminophylline[əmiːnəʊ'fɪliːn]n. 氨茶碱
adenosine[ə'denəsiːn]n. 腺苷
antagonist[æn'tæɡənɪst]n. 拮抗物,拮抗剂
intravenous[,ɪntrə'viːnəs]a. 静脉内的
sodium chloride['səʊdɪəm'klɔːraɪd] 氯化钠
hemodynamic[hiːməʊdaɪ'næmɪk]a. 血流动力学的
 Exercises
Exercises
Ⅰ.Reading Comprehension
A.Answer the following questions.
1.What are the clinical features of acute renal failure?
2.According to the passage,what may severe or prolonged hypoperfusion lead to?
3.What physical signs suggest prerenal ARF?
4.For ischemic or nephrotoxic ARF,why is prevention of paramount important?
5.In what condition is prerenal ARF reversible?
B.Choose the right answer to each question.
1.Prerenal ARF occurs in the setting of__________ .
A.thirst B.low cardiac output
C.renal hypoperfusion D.orthostatic dizziness
2.__________ can be avoided by close attention to cardiovascular function and intravascular volume in high-risk patients.
A.Ischemic ARF B.Prerenal ARF
C.Nephrotoxic ARF D.Postrenal ARF
3.Which of the following factor is not used to estimate the GFR in the Cockcroft-Gault formula?
A.Age. B.Weight. C.Race. D.Sex.
4.__________ is an effective preventive measure for contrast nephropathy.
A.Loop diuretics B.Mannitol C.Sodium chloride D.Hydration
5.To prevent radiocontrast nephropathy,__________ is associated with
significant side effects and should be discouraged.
A.N-acetylcysteine B.fenoldopam
C.sodium bicarbonate D.theophylline
Ⅱ.Words and Expressions
A.Fill in the blanks with the words or expressions given below,and change the form where necessary.
nephropathy incidence mortality hypoperfusion hypovolemia
malignancy obstruction serum metabolite intravenous
vasodilator cardiac ischemic necrosis hypertension
1.In states of mild__________ ,glomerular perfusion and the filtration fraction are preserved through several compensatory mechanisms.
2.Renal biopsy is particularly useful when clinical assessment and laboratory investigations suggest diagnoses other than__________ or nephrotoxic injury that may respond to disease-specific therapy.
3.Less common causes of acute lower urinary tract__________ include blood clots,calculi,and urethritis with spasm.
4.Approximately 5%of patients develop a transient salt-wasting syndrome that may require administration of__________ saline to maintain blood pressure.
5.Malignant__________ may result in ARF,often in association with hypertensive injury to other organs and may mimic glomerulonephritis in its other clinical manifestations.
6.Hypovolemia leads to a fall in mean systemic arterial pressure,which is detected as reduced stretch by arterial(e.g.carotid sinus)and__________ baroreceptors.
7.The in-hospital__________ rate among patients with ARF ranges from20%to 50%or more,depending on underlying conditions,and has declined only marginally over the past 15 years.
8.Peak__________ creatinine concentrations are observed after 3—5 days with contrast nephropathy and return to baseline after 5—7 days.
9.With most nephrotoxins,the__________ of ARF is increased in the elderly and in patients with preexisting chronic kidney disease,true or“effective”hypovolemia,or concomitant exposure to other toxins.
10.Contrast__________ is most common in individuals with preexisting chronic kidney disease,diabetes mellitus,congestive heart failure or multiple myeloma.
B.Fill in the blanks with the suitable words or expressions from each group.
Chronic kidney disease is disease that is slow to develop and usually does not show any symptoms until kidney damage is permanent.The National Kidney and Urologic Disease Information Clearinghouse,a federal agency, 1 that about 4.5%of people over age 20 have 2 kidney disease as indicated by tests that measure 3 function.The most common cause of chronic kidney disease in the United States is 4 .It accounts for between 33%and 40%of all new 5 of chronic kidney disease in the United States.In diabetes,the body cannot break down glucose(sugar).This extra glucose in the blood damages the 6 ,so that they no longer filter 7 effectively.
High or uncontrolled blood pressure( 8 )is the second leading cause of chronic kidney disease.It accounts for between 27%and 30%of all new cases of chronic kidney disease.High blood pressure damages the 9 in the nephron,so that they can no longer work with the 10 to filter the blood.
Glomerulonephritis(肾小球肾炎)is a term for several different chronic kidney diseases where 11 to the nephrons causes 12 or red blood cells pass into the 13 .Kidney cancer is uncommon,accounting for only 2%of 14 cases.
Over-the-counter analgesics (pain medications)such as aspirin, acetaminophen(对乙酰氨基酚),ibuprofen(布洛芬),and similar 15 that can be bought without a 16 may make kidney disease worse in individuals who already have kidney damage or cause kidney damage in healthy individuals who take these medications daily for several years.The chance of damage is increased when these pain medications are taken in 17 with each other or with caffeine or codeine(Some painkilling 18 are a combination of pain medications and caffeine or codeine).Individuals who take these 19 regularly or who have been told they have kidney damage should discuss the risk of these medications with their 20 .
1.A.assesses B.evaluates C.calculates D.estimates
2.A.acute B.permanent C.chronic D.slow
3.A.lung B.kidney C.spleen D.gallbladder
4.A.heart attack B.renal failure C.hypotension D.diabetes
5.A.cases B.examples C.instances D.conditions
6.A.liver B.vessel C.nephrons D.renal glomerulus
7.A.urine B.blood C.bile D.marrow
8.A.hypertension B.pressure C.stress D.hypotension
9.A.blood vessels B.pulse C.artery D.capillaries
10.A.arteries B.tubules C.veins D.nerves
11.A.damage B.injury C.cut D.wound
12.A.nutrient B.white blood cells C.glucose D.protein
13.A.blood B.urine C.serum D.saliva
14.A.cancer B.disease C.death D.tumor
15.A.antibiotics B.vitamins C.medications D.herbal medicines
16.A.instruction B.prescription C.recommendation D.direction
17.A.cooperation B.coordination C.combination D.accordance
18.A.analgesics B.aspirin C.tablets D.medicine
19.A.ointments B.capsules C.caffeine D.painkillers
20.A.physician B.intern C.pharmacist D.surgeon
Ⅲ.Translation
A.Translate the following sentences into Chinese.
1.More severe or prolonged hypoperfusion may lead to ischemic injury,often termed acute tubular necrosis,or ATN.Thus,prerenal ARF and ischemic ATN fall along a spectrum of manifestations of renal hypoperfusion. Prerenal ARF can complicate any disease that induces hypovolemia,low cardiac output,systemic vasodilatation,or selective intrarenal vasoconstriction.
2.Because there are no specific therapies for ischemic or nephrotoxic ARF, prevention is of paramount importance.Many cases of ischemic ARF can be avoided by close attention to cardiovascular function and intravascular volume in high-risk patients,such as the elderly and those with preexisting chronic kidney disease.
3.However,aside from the potential hazards associated with a delay in radiographic imaging,N-acetylcysteine appears to be safe,and its use in patients at high risk for radiocontrast nephropathy is reasonable,based on its low side effect profile.Larger RCTs will be required to show definitive benefit.
B.Translate the following sentences into English.
1.诊断肾衰竭患者的第一步是确定其肾衰竭属急性还是慢性。如果化验结果分析显示血尿素氮和肌酐水平升高是近期出现的,这就表明该病变过程为急性肾衰竭。
2.无尿表明尿道完全梗阻,但可能会并发严重的肾前性或肾性急性肾衰竭。尿排出量大幅增减加大了间歇性梗阻的可能性,而尿道部分梗阻患者可能会出现多尿症状,这是由于尿浓缩机制受损所致。
Ⅳ.Writing
A.Write an abstract of Text A.
B.Write a topic-related and literature-based report on Acute Renal Failure.